Ablation of the Ablator: Accidental Guide Catheter Machining by a 1.75-mm Burr in a 6F Amplatz Guide
© 2026 HMP Global. All Rights Reserved.
Any views and opinions expressed are those of the author(s) and/or participants and do not necessarily reflect the views, policy, or position of the Journal of Invasive Cardiology or HMP Global, their employees, and affiliates.
J INVASIVE CARDIOL 2026. doi:10.25270/jic/26.00032. Epub February 4, 2026.
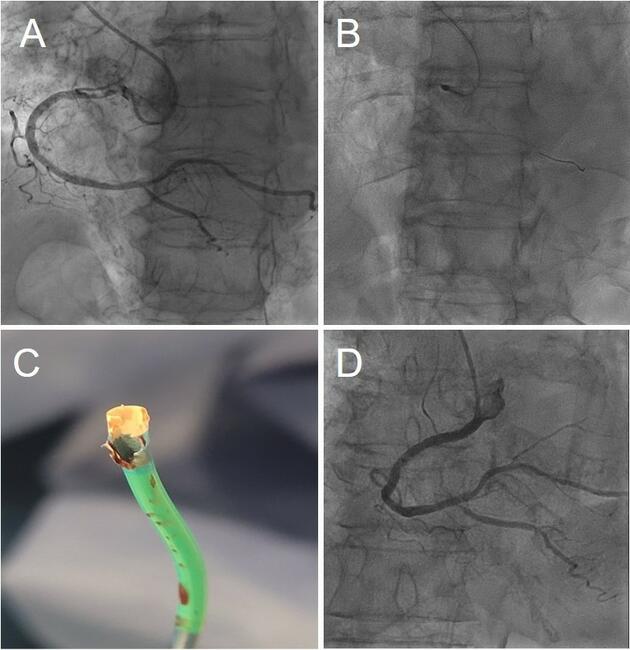
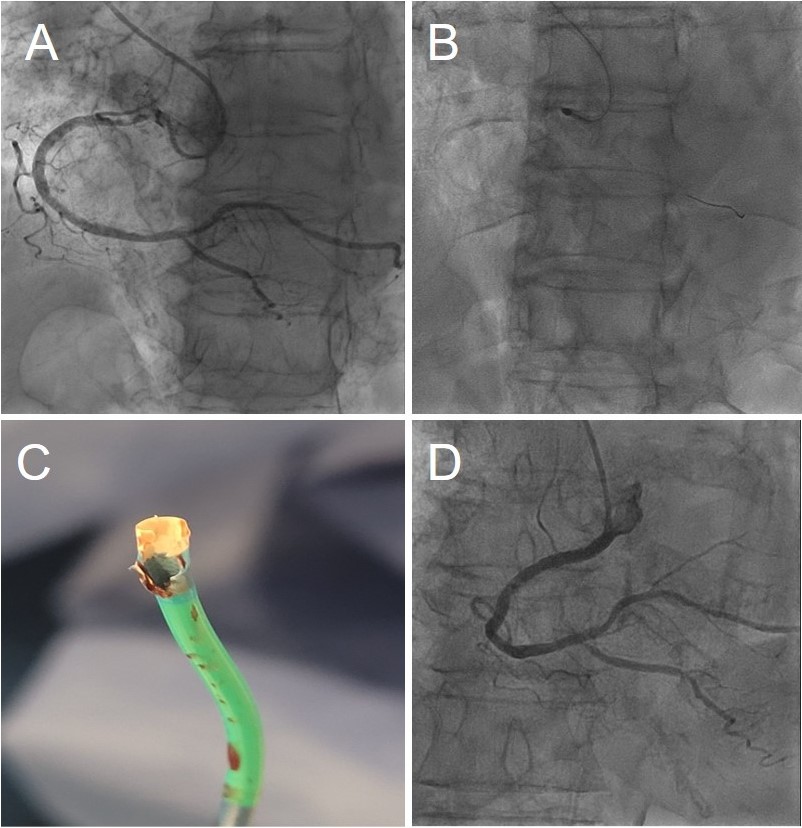
An 85-year-old woman presented with a subocclusive (99%), severely calcified ostial lesion of the right coronary artery (RCA) (Figure A, Video 1). A 6F Launcher Amplatz Left (AL) 0.75 guide catheter (Medtronic) (inner diameter: 1.80 mm/0.071 in) was selected to maximize back-up support. After wire exchange for a RotaWire (Boston Scientific) using a 1.9F Caravel microcatheter (ASAHI INTECC), rotational atherectomy (RA) was initiated with a 1.75-mm burr. Although standard best practice is to initiate RA with a 1.5-mm burr to minimize the risk of burr entrapment and allow stepwise lesion reassessment,1 a 1.75-mm burr was selected upfront in this case to achieve a burr-to-artery ratio closer to 0.5, aiming for optimal plaque modification in a large-caliber vessel (approximately 4.5 mm).
Given the severity of the ostial lesion and immediate resistance at the coronary inlet, RA was initiated close to the distal tip of the guide catheter, requiring a careful millimeter-by-millimeter advancement with multiple short runs (total cumulative burr time: 75 seconds). After these initial incremental passes, a final run was performed, as illustrated in Video 2. Following atherectomy, intravascular lithotripsy (IVL) could have been considered as part of a rota-lithotripsy strategy; however, a “Rota-Cut” approach was favored, as the prolonged balloon inflations required for IVL might be poorly tolerated in a very dominant RCA. Shorter inflation with a cutting balloon were therefore preferred to maintain hemodynamic stability, while also offering a more cost-effective approach. The lesion was then further prepared using a 3.5 × 10-mm Wolverine cutting balloon (Boston Scientific) with a single inflation at a maximum pressure of 16 atm for a total duration of 20 seconds. A double-wire technique—1 wire positioned in the ascending aorta for stability and 1 in the RCA—was subsequently used to deliver and accurately position a 4.0 by 24-mm Synergy Megatron stent (Boston Scientific) (Video 3).
The complication remained clinically silent until the end of the procedure, when unexpected resistance was encountered during stent balloon retrieval. Withdrawal of the system revealed catastrophic structural damage of the guide catheter tip (Figure C); the polymer soft tip of the Launcher was extensively machined and charred, with complete exposure of the internal stainless-steel braiding. Final angiography after high-pressure optimization to 4.60 mm showed an excellent result with Thrombolysis in Myocardial Infarction-3 flow (Figure D, Video 4). At the 8-month clinical follow-up, the patient remained asymptomatic.
This case illustrates the “1:1 ratio trap” in RA: a 1.75-mm (0.0689 in) burr within a 6F guide catheter (1.80 mm/0.071 in) leaves a theoretical clearance of only 0.05 mm (0.002 in), providing virtually no safety margin.2-4
- Ostial engagement challenge: In subocclusive ostial lesions, initiating burr rotation close to the guide tip may be unavoidable to gain coronary entry. However, this case demonstrates that even careful, incremental advancement under these conditions can induce progressive internal machining of the guide catheter wall.
- Guide size requirement: For lesions requiring ablation at or from the guide tip, a 7F system (inner diameter: 2.06 mm/0.081 in) should be preferred, providing a substantially larger clearance (~ 0.31 mm) and reducing the risk of burr-catheter interaction (2).
- Shape constraint: Aggressive guide shapes such as the AL induce distal curvature and eccentric alignment (Figure B, Video 2), effectively abolishing the minimal clearance and allowing the high-speed burr to behave like an industrial lathe against the catheter wall.
- Role of the double-wire technique: The additional aortic wire was primarily used to optimize support and stent positioning at the ostium. Retrospective analysis of the fluoroscopic sequences during this step (Video 3) revealed abnormal widening of the guide tip, which was only correctly interpreted after catheter retrieval.
Affiliations and Disclosures
Kaïs Ouerghi, MD¹; Victor Mateus, MD¹; Tahar Lazizi, MD¹; Loïc Bière, MD, PhD²
From the ¹Department of Interventional Cardiology, Laval Hospital, Laval, France; ²Department of Interventional Cardiology, University Hospital of Angers (CHU d’Angers), Angers, France.
Disclosures: The authors report no financial relationships or conflicts of interest regarding the content herein.
Consent statement: The authors confirm that informed consent was obtained from the patient for the interventions described in the manuscript and for the publication of the patient’s data, including all images and videos.
Address for correspondence: Kaïs Ouerghi, MD, Department of Interventional Cardiology, Centre Hospitalier de Laval 33 Rue du Haut Rocher, Laval 53000, France. Email: ouerghi_kais@hotmail.fr
References
- Tomey MI, Kini AS, Sharma SK. Current status of rotational atherectomy. JACC Cardiovasc Interv. 2014;7(4):345-353. doi:10.1016/j.jcin.2013.12.196
- Barbato E, Carrié D, Dardas P, eet al; European Association of Percutaneous Cardiovascular Interventions. European expert consensus on rotational atherectomy. EuroIntervention. 2015;11(1):30-36. doi:10.4244/EIJV11I1A6
- Medtronic. Launcher guide catheter 6F. 2023. Accessed January 25, 2026. https://www.medtronic.com/content/dam/medtronic-wide/public/united-states/products/cardiac-vascular/cardiovascular/coronary-catheters/launcher-6f-product-specifications1.pdf
- Medtronic. Launcher guide catheter 7F. 2023. Accessed January 25, 2026. https://www.medtronic.com/content/dam/medtronic-wide/public/united-states/products/cardiac-vascular/cardiovascular/coronary-catheters/launcher-7f-product-specifications1.pdf