

Percutaneous Retrieval of an Intracardiac Fractured Vascular Access Port Catheter Using a Looped Guidewire
© 2025 HMP Global. All Rights Reserved.
Any views and opinions expressed are those of the author(s) and/or participants and do not necessarily reflect the views, policy, or position of the Journal of Invasive Cardiology or HMP Global, their employees, and affiliates.
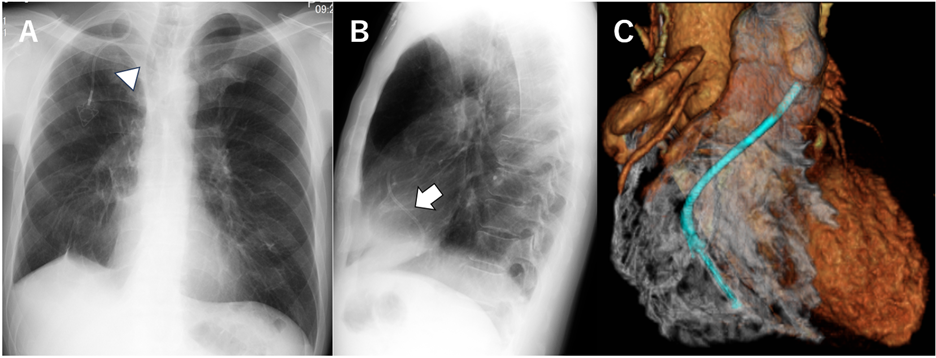
A 47-year-old man with a history of chemotherapy for metastatic gastric cancer was incidentally found on chest X-ray to have a fractured vascular access port catheter in the right heart, which had been intact 10 months earlier. Computed tomography revealed that one end of the catheter was located in the right ventricular outflow tract, while the other extended through the tricuspid valve into the coronary sinus (Figure A-C).
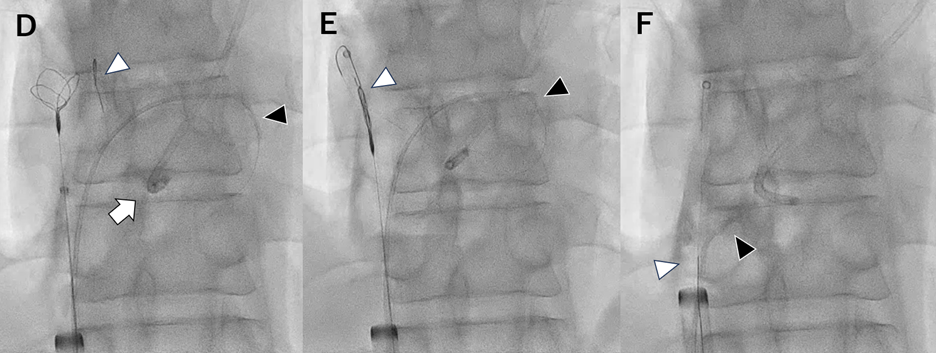
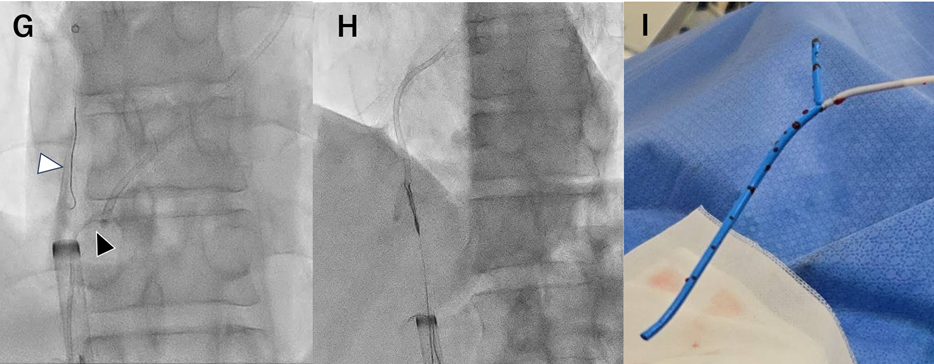
The patient was referred for percutaneous retrieval. Venous access was obtained via the right common femoral vein, and an 18F long sheath was introduced. A 5F Judkins Left-1 diagnostic catheter was used to advance a shaped 0.014-inch floppy guidewire (Cruise; ASAHI INTECC) to loop around and encircle the fractured catheter. The guidewire was then grasped using a 9- to 15-mm Atrieve multiloop snare (Argon Medical Devices) inserted through the same sheath. Closure of the snare successfully trapped the fractured catheter, which was pulled toward the sheath. As the catheter moved into the sheath, it was directly grasped with the snare and completely retrieved (Figure D-I, Videos 1 and 2).
Directly grasping foreign bodies with devices is a common retrieval method. However, when the object is distant or difficult to access, using a looped guidewire can effectively facilitate entrapment and retrieval.
Affiliations and Disclosures
Kazuhiro Asano, MD; Tatsuya Nakama, MD; Kotaro Obunai, MD
From the Department of Cardiology, Tokyo Bay Urayasu Ichikawa Medical Center, Urayasu, Chiba, Japan.
Disclosures: The authors have no financial relationships or conflicts of interest regarding the content.
Consent statement: The authors confirm that informed consent was obtained from the patient for the images described in the manuscript and for the publication.
Address for correspondence: Kazuhiro Asano, MD, Department of Cardiology, Tokyo Bay Urayasu Ichikawa Medical Center, 3-4-32, Todaijima, Urayasu, Chiba 279-0001, Japan. Email: kaz-asano@nms.ac.jp











