


Routine Coronary Procedures via Distal Transradial Access in Male Versus Female Patients: Insights From the DISTRACTION Registry
© 2025 HMP Global. All Rights Reserved.
Any views and opinions expressed are those of the author(s) and/or participants and do not necessarily reflect the views, policy, or position of the Journal of Invasive Cardiology or HMP Global, their employees, and affiliates.
Abstract
Objectives. Systematic reviews and meta-analyses have highlighted the benefits of distal over proximal transradial access, including lower rates of radial artery occlusion and faster hemostasis. Despite the increasing adoption of distal transradial access by interventionalists, there is a lack of data addressing gender-specific differences. This study aimed to assess those differences in routine coronary procedures via distal transradial access.
Methods. The authors conducted a retrospective analysis of a large, real-world sample of 6871 consecutive all-comers who underwent coronary procedures via distal transradial access using data from the DISTRACTION registry.
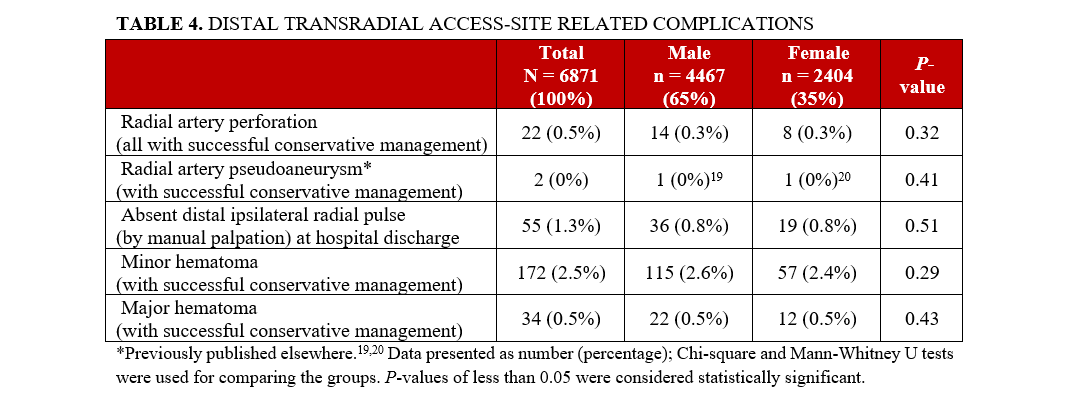
Results. The mean patient ages were 63.8 ± 15.7 years, 63.5 ± 17.7 years, and 64.4 ± 11.1 years for total, male, and female groups, respectively; 65% of the patients were male. In the female group, there was statistically significant predominance of hypertension (82.2% vs 74%), diabetes (46.8% vs 37%), obesity (29.3% vs 22.2%), severe mitral valve disease (3.1% vs 1.1%), coronary angiography-only (48.7% vs 36%), and access site crossovers (3.1% vs 1.5%). In the male group, there were more rates of former or current smoking (54.2% vs 40.8%), previous percutaneous coronary intervention (PCI) (29.8% vs 19.7%), previous coronary artery bypass grafting (4.5% vs 1.9%), ST-segment elevation myocardial infarction (24.2% vs 18.5%), PCI (66.1% vs 52.5%), left main PCI (2.6% vs 1.7%), redo right distal transradial access (15.3% vs 9.9%), and 7F sheath size (2.6% vs 0.9%). No major adverse cerebrovascular and cardiac events directly related to distal transradial access, no hand/thumb dysfunction or ischemia after any procedure, and no relevant access site-related bleeding were recorded.
Conclusions. The adoption of distal transradial access by proficient operators as the default approach for routine coronary procedures appears to be safe and feasible in both male and female patients, with very low rates of access site crossovers and complications.
Introduction
Compared with proximal, traditional, or conventional access, distal transradial access has advantages such as faster hemostasis as well as lower rates of proximal radial artery occlusion,1-3 which is the most frequent complication of proximal transradial access.4
Performing coronary angiography or percutaneous coronary intervention (PCI) via proximal transradial access is technically more challenging in females than males, mainly because of increased rates of radial artery spasm and smaller radial arteries.5 In Korean patients, the mean distal radial artery diameter has been shown to be approximately 20% smaller than the proximal diameter,6 and females have significantly smaller diameters of distal radial arteries than males.5,6 Since February 2019, our group has adopted distal transradial access as the default for routine coronary angiography and/or PCI, and our results have been previously published.7-16
Despite the increasing incorporation of distal transradial access by interventionalists around the world, there is a lack of data about sex differences in coronary procedures via distal transradial access. In this study, we aimed to assess those differences in routine coronary angiography and/or PCI via distal transradial access from a large-scale, real-world registry of consecutive, all-comer patients.
Methods
From February 2019 to July 2024, 6871 consecutive patients who underwent coronary angiography and/or PCI via distal transradial access at Hospital São Paulo, Escola Paulista de Medicina, Universidade Federal de São Paulo, São Paulo, Brazil were enrolled in the DISTRACTION (DIStal TRAnsradial access as default approach for Coronary angiography and intervenTIONs) registry (ensaiosclinicos.gov.br identifier: RBR-7nzxkm). The presence of any (even weak) palpable pulses at both proximal and distal radial arteries was the eligibility criterion for enrollment. Of note, patients with unstable hemodynamic conditions were not excluded. The study was approved by the Research Ethics Committee, Hospital Universitário I, Universidade Federal de São Paulo (protocol 4.071.731), CAAE 30384020.5.0000.5505, and informed consent was given as a prerequisite before enrolling each patient in this registry. The study was conducted in accordance with the Declaration of Helsinki (as revised in 2013). Our standardized protocol for distal transradial access procedures has been extensively described elsewhere.7,9,10
Statistical analysis
Study data were collected and managed using Research Electronic Data Capture (REDCap) version 15.4.0 (Vanderbilt University), hosted at Escola Paulista de Medicina. REDCap is a secure, web-based software platform designed to support data capture for research studies, providing (1) intuitive interface for validated data capture, (2) audit trails for tracking data manipulation and export procedures, (3) automated export procedures for seamless data downloads to common statistical packages, and (4) procedures for data integration and interoperability with external sources.17,18
Continuous variables were described as mean ± SD and categorical data as numbers and percentages. Chi-square and Mann-Whitney U tests were used for comparing the groups; P-values of less than 0.05 were considered statistically significant. All analyses were performed with the BioStat Biology Statistical Software for Windows, version 5.4 (Analyst Soft, Inc.).
Results
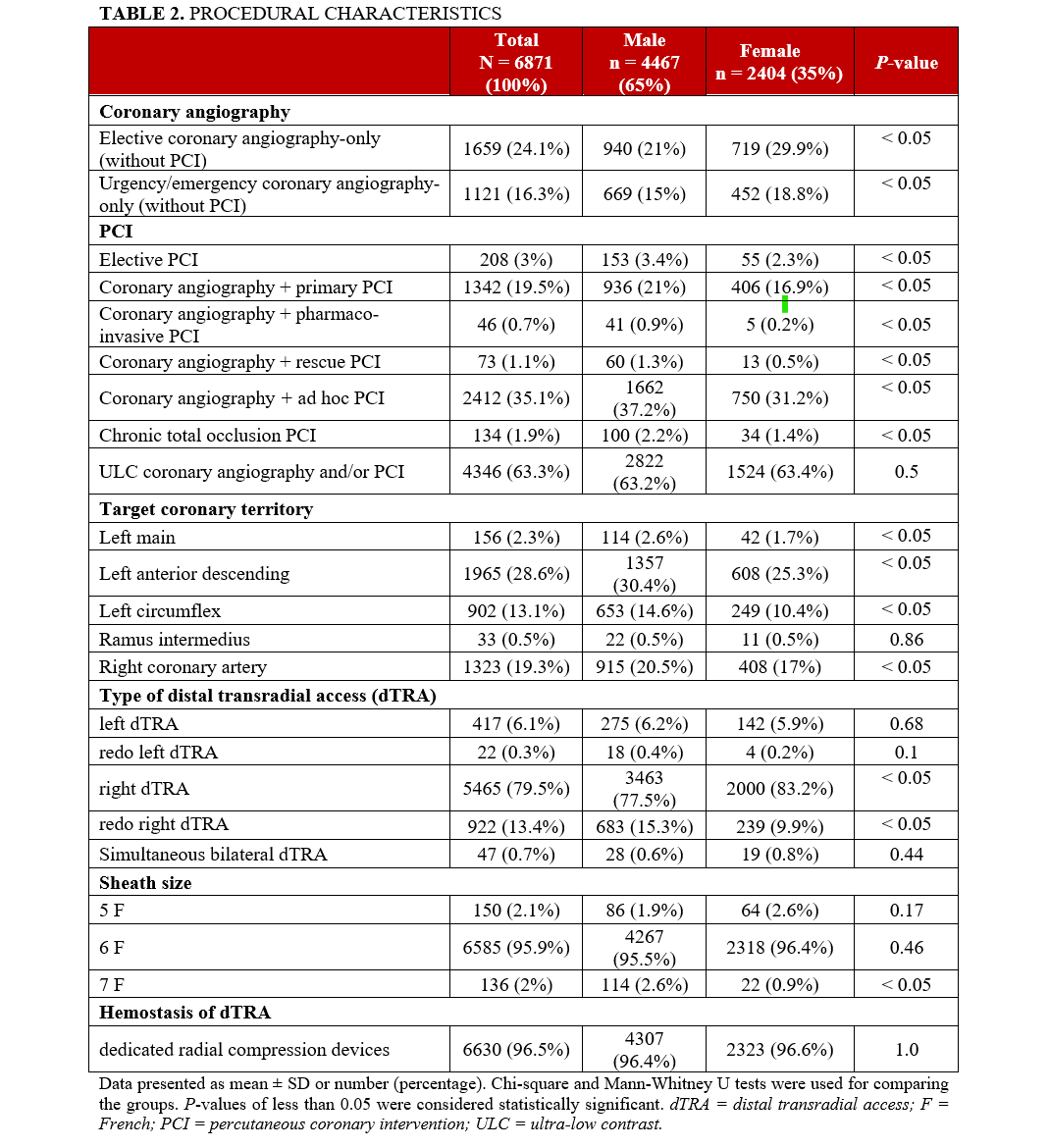
Table 1 depicts the baseline demographic features and Table 2 presents the procedural characteristics of all 6871 patients according to each group. Overall, there was a predominance of males (n = 4467, 65%). The mean patient ages were 63.8 ± 15.7, 63.5 ± 17.7, and 64.4 ± 11.1 years, for total, male, and female groups, respectively.

In the female group (n = 2404, 35%), there was statistically significant predominance of hypertension (82.2% vs 74%; P < .05), diabetes (46.8% vs 37%; P < .05), obesity (29.3% vs 22.2%; P < .05), and severe mitral valve disease (3.1% vs 1.1%; P < .05). In the male group, there were more statistically significant rates of former or current smoking (54.2% vs 40.8%; P < .05); previous PCI (29.8% vs 19.7%; P < .05); previous coronary artery bypass graft surgery (4.5% vs 1.9%; P < .05); previous ipsilateral proximal (11.8% vs 8%; P < .05) or distal (15.8% vs 10.3%; P < .05) transradial sheath insertion, and total (24.2% vs 18.5%; P < .05), anterior (11.8% vs 9.1%; P < .05), or inferior (9.7% vs 7%; P < .05) ST-segment elevation myocardial infarction (STEMI) (Table 1).
Regarding procedural characteristics, the rates of coronary angiography-only (without any type of intervention) were statistically significantly higher in the female group than in the male group (48.7% vs 36%; P < .05). In the male group, there was statistically significant predominance of the total amount of PCI (66.1% vs 52.5%; P < .05); left main (2.6% vs 1.7%; P < .05), left anterior descending (30.4% vs 25.3%; P < .05), left circumflex (14.6% vs 10.4%; P < .05), and right coronary PCI (20.5% vs 17%; P < .05); redo right distal transradial access (15.3% vs 9.9%; P < .05); and 7F sheath usage (2.6% vs 0.9%; P < .05) (Table 2).
Right distal transradial access (89.5%), standard 6F radial sheaths (94.1%), and hemostasis by dedicated radial compression devices (95.2%) were performed for the vast majority of patients in both groups. The total access site crossover was very low (2%), with statistically significant predominance in female compared with male patients (3.1% vs 1.5%; P < .05), most of which were successfully performed via any proximal or contralateral distal transradial access (Table 3).
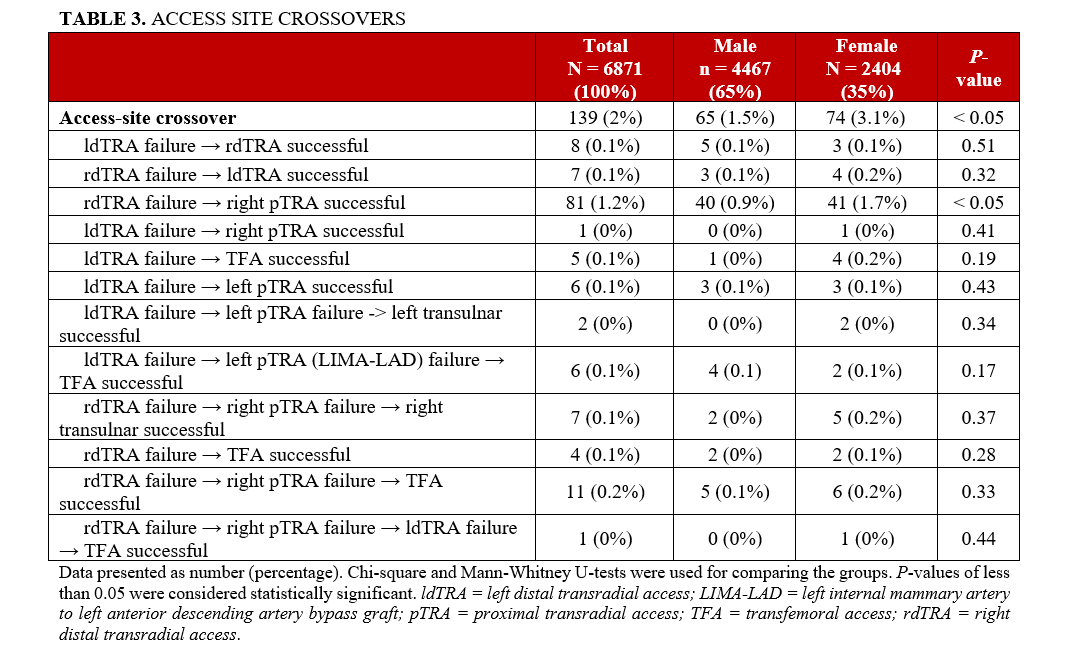
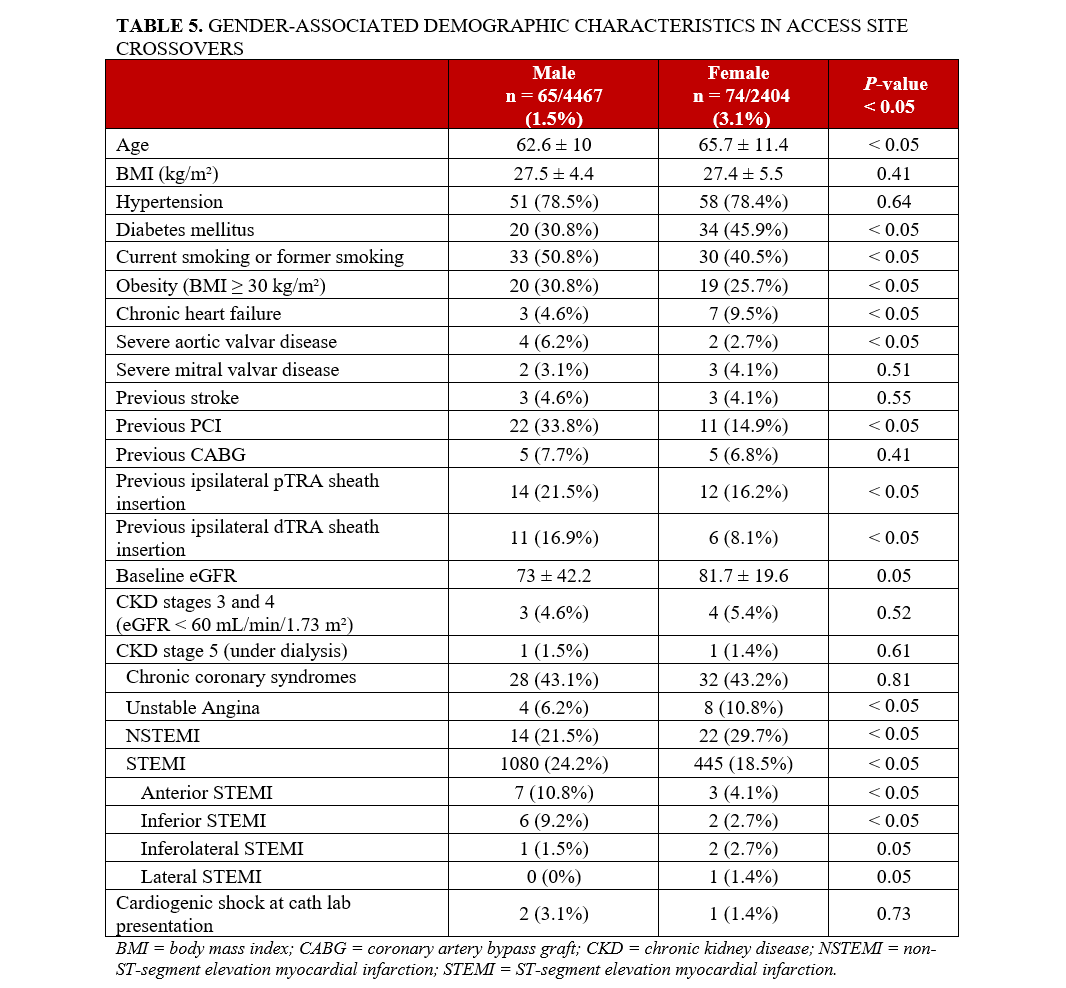
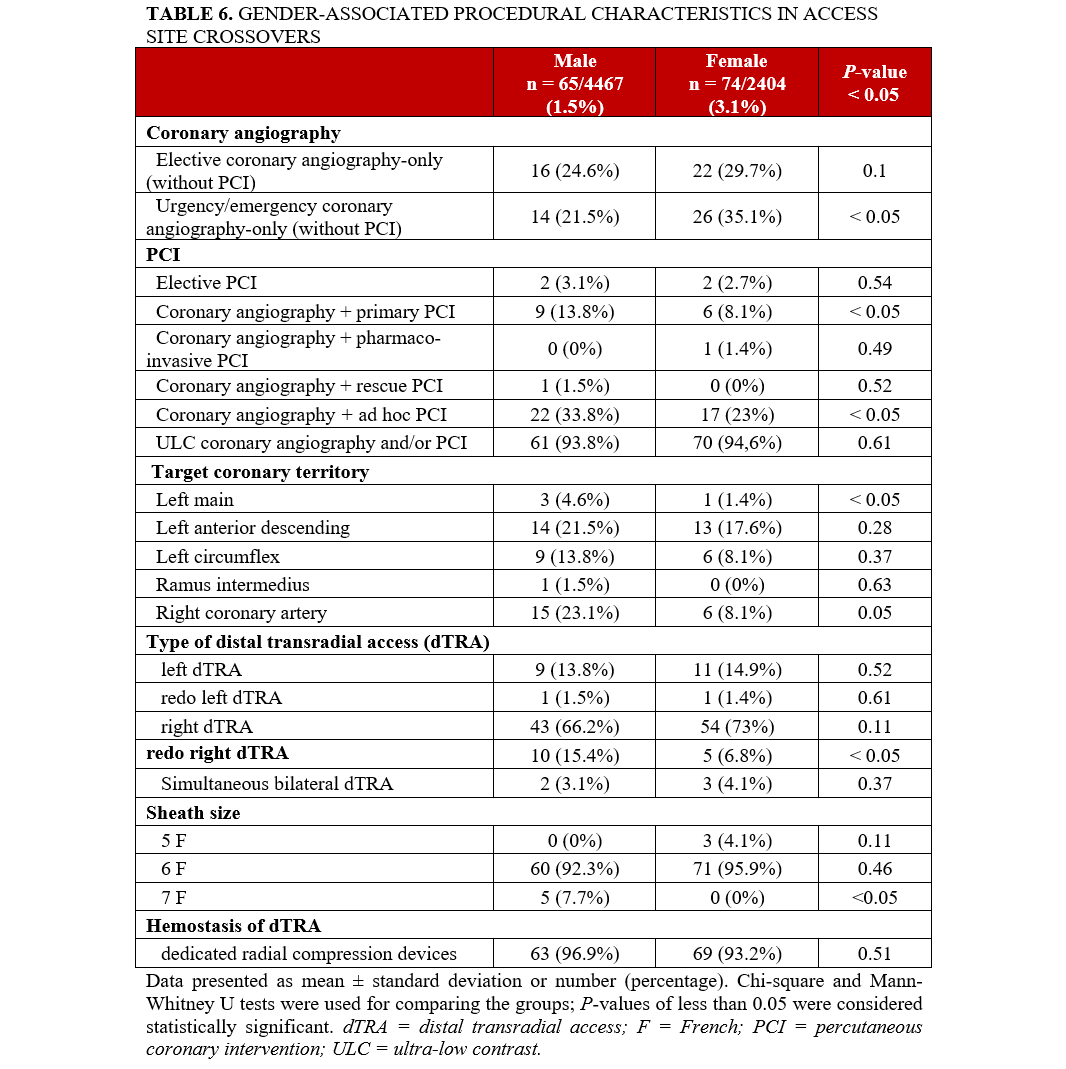
Table 4 depicts specific procedural-related complications,19,20 and Tables 5 and 6 present gender-associated characteristics in access site crossovers.
Discussion
The present study assessed gender-related particularities of routine coronary angiography and/or PCI via distal transradial access, from a large, unselected and real-world sample of all-comers patients, encompassing all presentations of coronary artery disease. Data were obtained from the DISTRACTION, the first Brazilian registry to address this issue.
Kim et al5 evaluated 117 Korean patients submitted to coronary angiography and/or PCI via left distal transradial access. Left radial artery angiography was achieved from 101 patients, 69 (68.3%) male and 32 (31.7%) female. The average diameter of distal radial artery was 2.57 mm. Female patients, compared with male, had a significantly smaller diameter of distal radial artery (2.40 vs 2.65 mm, P = .016). Nevertheless, coronary angiography and/or PCI were successfully performed in all 117 patients, with 6F sheaths. There was nonsignificant lower success rate for female patients, in comparison to male (84.2% vs 91.1%, P = .264). In our registry, due to logistic reasons, distal and proximal radial artery diameters were not routinely measured, neither by ultrasound nor by angiography.
Lee at al6 used ultrasound to assess the bilateral proximal and distal radial artery diameters of 1162 consecutive Korean patients. The mean distal radial artery diameters were 2.31 ± 0.43 mm (right) and 2.35 ± 0.45 mm (left). The distal radial artery was significantly smaller in female than in male patients (right: 2.15 ± 0.38 mm vs 2.43 ± 0.44 mm, P < 0.001; left: 2.18 ± 0.39 mm vs 2.47 ± 0.45 mm, P < 0.001). The mean distal radial artery diameter was approximately 20% smaller than that of the proximal. A total of 630 (54.2%) and 574 (49.4%) patients had a distal radial artery diameter of less than 2.3 mm in the right and left hands, respectively; these were mainly female patients with a low body mass index and body surface area. No data related to coronary angiography or PCI was reported.
In the DATA-STAR study,19 a retrospective analysis of the safety and efficacy of 545 patients undergoing coronary procedures via right distal (263 patients) or right proximal (282 patients) transradial access, all patients underwent preprocedural ultrasound of their arm arteries; all patients had a radial artery diameter of less than 2.1 mm (mean: 1.63 ± 0.27 mm). The baseline characteristics were similar between groups. The primary endpoint of puncture success was significantly lower in the distal transradial access group (79.5% vs 98.5%, P < .0001); puncture success was also lower in the subgroup of patients with a radial artery diameter of less than 1.6 mm (vs > or ≥ 1.6 mm) in the distal transradial access group (P < .0001). The puncture time was significantly higher (2.1 ± 1.4 vs 1.0 ± 0.45 min, P < .00001) in the distal transradial access group. Vascular access site complications (including access site hematomas) and radial artery occlusion at 1 day and at 1 month after the procedure were similar between the 2 groups.
In contrast to most data published to date1,2—which largely included patients at stable conditions—we have been continuously including patients with any (even weak) distal (and proximal) radial artery palpable pulses, no matter the clinical scenario. Of note, the majority of our patients presented with acute coronary syndromes (55.2%, 56.8%, and 52.1% for total, male, and female groups, respectively). Despite the statistically significant predominance of classic coronary risk factors in female patients, in male patients we observed higher rates of established coronary artery disease based on previous percutaneous or surgical revascularization, as well as more acute coronary syndromes at presentation, mainly STEMI, that required further PCI, compared with female patients.
In the KODRA (Korean Prospective Registry for Evaluating the Safety and Efficacy of Distal Radial Approach) registry,20 the rates of access site crossover occurred in 333 of 4977 (6.7%) patients. In the DISTRACTION registry, access site crossover decreased from 3% in our very early experience7 to 2.5% after 3 years, with 8.5 times the initial number of patients;10 this number dropped to 2% after 5 years and reaching 6800 consecutive patients.13,14 In this present analysis of 6871 patients, the total access site crossover rate remained very low (2%), with statistically significant predominance in female compared with male patients (3.1% vs 1.5%; P < .05). The majority of distal transradial access crossover was successfully performed via proximal or contralateral distal transradial access, thus avoiding the transfemoral approach.
Limitations
This is an observational registry, and all procedures were performed by 2 interventional cardiologists who were experienced with distal transradial access. There are particularities that may be specific to the population under study, even though this was an all-comer population; the 2 groups were not comparable at baseline and the data cannot provide any meaningful conclusions on procedural parameters or outcomes in females compared with males. Thus, the results of the present study should not be extrapolated or generalized to other centers and to interventional cardiologists unfamiliar with the technique. Distal radial artery punctures were not performed under ultrasound guidance, and no distal or proximal radial artery diameter measurements were evaluated before or after the procedures. Distal radial artery puncture attempts, time-to-sheath insertion, and fluoroscopy and procedure times were not systematically recorded. The lack of routine post-procedure Doppler ultrasound evaluation might have underestimated vascular complication rates.
Conclusions
The adoption of distal transradial access as the default approach for routine coronary procedures by proficient operators appears to be safe and feasible in both male and female patients, with very low rates of access site crossovers and complications.
Affiliations and Disclosures
Marcos Danillo Oliveira, MD, MSc; Adriano Caixeta, MD, PhD
From the Department of Interventional Cardiology, Hospital Universitário I, Escola Paulista de Medicina, Universidade Federal de São Paulo, São Paulo-SP, Brazil.
Disclosures: The authors report no financial relationships or conflicts of interest regarding the content herein.
Address for correspondence: Adriano Caixeta, MD, PhD, Department of Interventional Cardiology, Hospital São Paulo, Escola Paulista de Medicina, UNIFESP, R. Napoleão de Barros, 715 - Vila Clementino, São Paulo-SP 04024-002, Brazil. Email: acaixeta@me.com
References
1. Ferrante G, Condello F, Rao SV, et al. Distal vs conventional radial access for coronary angiography and/or intervention: a meta-analysis of randomized trials. JACC Cardiovasc Interv. 2022;15(22):2297-2311. doi:10.1016/j.jcin.2022.09.006
2. Feghaly J, Chen K, Blanco A, Pineda AM. Distal versus conventional radial artery access for coronary catheterization: a systematic review and meta-analysis. Catheter Cardiovasc Interv. 2023;101(4):722-736. doi:10.1002/ccd.30602
3. Oliveira MD, Caixeta A. Distal transradial access to prevent proximal radial artery occlusion: what is really known? J Transcat Interv. 2021;29:eA202102. doi:10.31160/JOTCI202129A202102
4. Sgueglia GA, Di Giorgio A, Gaspardone A, Babunashvili A. Anatomic basis and physiological rationale of distal radial artery access for percutaneous coronary and endovascular procedures. JACC Cardiovasc Interv. 2018;11(20):2113-2119. doi:10.1016/j.jcin.2018.04.045
5. Kim Y, Ahn Y, Kim MC, al. Gender differences in the distal radial artery diameter for the snuffbox approach. Cardiol J. 2018;25(5):639-641. doi:10.5603/CJ.2018.0128
6. Lee JW, Son JW, Go TH, et al. Reference diameter and characteristics of the distal radial artery based on ultrasonographic assessment. Korean J Intern Med. 2022;37(1):109-118. doi:10.3904/kjim.2020.685
7. Oliveira MDP, Navarro EC, Kiemeneij F. Distal transradial access as default approach for coronary angiography and interventions. Cardiovasc Diagn Ther. 2019;9(5):513-519. doi:10.21037/cdt.2019.09.06
8. Oliveira MDP, Caixeta A. Distal transradial access (dTRA) for coronary angiography and interventions: a quality improvement step forward? J Invasive Cardiol. 2020;32(9):E238-E239. doi:10.25270/jic/20.00160
9. Oliveira MDP, Navarro EC, Caixeta A. Distal transradial access for post-CABG coronary and surgical grafts angiography and interventions. Indian Heart J. 2021;73(4):440-445. doi:10.1016/j.ihj.2021.06.005
10. Oliveira MD, Navarro EC, Caixeta A. Distal transradial access for coronary procedures: a prospective cohort of 3,683 all-comers patients from the DISTRACTION registry. Cardiovasc Diagn Ther. 2022;12(2):208-219. doi:10.21037/cdt-21-542
11. Oliveira MD, Caixeta A. Distal transradial access for primary PCI in ST-segment elevation myocardial infarction. JACC Cardiovasc Interv. 2022;15(7):794-795. doi:10.1016/j.jcin.2022.02.021
12. Oliveira MD, Navarro EC, Branca NR, Garcia ME, Scarpa MC, Caixeta A. Coronary procedures via distal transradial access in older as compared with non-older patients: insights from the DISTRACTION registry. J Invasive Cardiol. 2023;35(9). doi:10.25270/jic/23.00132
13. Oliveira MD, Motta RFOS, Caixeta A. Distal transradial access for coronary procedures: insights from 6,800 consecutive all-comers patients from the DISTRACTION registry. Int J Cardiovasc Sci. 2024;37:e20240084. doi:10.36660/ijcs.20240084
14. Oliveira MD, Motta RS, Oliveira LC, Caixeta A. Distal transradial access for coronary procedures: insights from 6,852 consecutive all-comers patients from the DISTRACTION registry. J Am Coll Cardiol. 2025;85(12):906.
15. Oliveira MD, Motta RS, Oliveira LC, Caixeta A. Ultra-low contrast strategy for routine coronary procedures: insights from the DISTRACTION (distal transradial access as default for coronary angiography and interventions) registry. J Am Coll Cardiol. 2025;85(12):1016.
16. Oliveira MD, Caixeta A. Ultra-low contrast strategy for routine coronary procedures via distal transradial access: real-world experience with consecutive all-comers patients from the DISTRACTION registry. J Invasive Cardiol. 2025;37(4). doi:10.25270/jic/24.00276
17. Harris PA, Taylor R, Thielke R, Payne J, Gonzalez N, Conde JG. Research electronic data capture (REDCap)--a metadata-driven methodology and workflow process for providing translational research informatics support. J Biomed Inform. 2009;42(2):377-381. doi:10.1016/j.jbi.2008.08.010
18. Harris PA, Taylor R, Minor BL, et al; REDCap Consortium. The REDCap consortium: Building an international community of software platform partners. J Biomed Inform. 2019;95:103208. doi:10.1016/j.jbi.2019.103208
19. Oliveira MD, Perillo P, Lemos L, Caixeta A. Prolonged Doppler US-guided pneumatic compression of a radial artery pseudoaneurysm after percutaneous coronary intervention: a simple and effective solution for a rare and challenging problem. J Vasc Bras. 2023;22:e20210212. doi:10.1590/1677-5449.202102122
20. Oliveira MDP, Alves de Sá G, Navarro EC, Caixeta A. Pseudoaneurysm after distal transradial coronary intervention successfully managed by prolonged pneumatic compression: simple solution for a rare and challenging problem. J Invasive Cardiol. 2021;33(10):E836-E838. doi:10.25270/jic/21.00139
21. Chugh Y, Kanaparthy NS, Piplani S, et al. Comparison of distal radial access versus standard transradial access in patients with smaller diameter radial arteries(The distal radial versus transradial access in small transradial arteriesstudy: D.A.T.A - S.T.A.R study). Indian Heart J. 2021;73(1):26-34. doi:10.1016/j.ihj.2020.11.002
22. Lee JW, Kim Y, Lee BK, et al. Distal radial access for coronary procedures in a large prospective multicenter registry: the KODRA trial. JACC Cardiovasc Interv. 2024;17(3):329-340. doi:10.1016/j.jcin.2023.11.021










