Catastrophic Right Coronary Artery Dissection After Surgical Removal of Coronary Chimney Stents Following Valve-in-Valve Transcatheter Aortic Valve Implantation
© 2026 HMP Global. All Rights Reserved.
Any views and opinions expressed are those of the author(s) and/or participants and do not necessarily reflect the views, policy, or position of the Journal of Invasive Cardiology or HMP Global, their employees, and affiliates.
J INVASIVE CARDIOL 2026. doi:10.25270/jic/26.00074. Epub April 7, 2026.
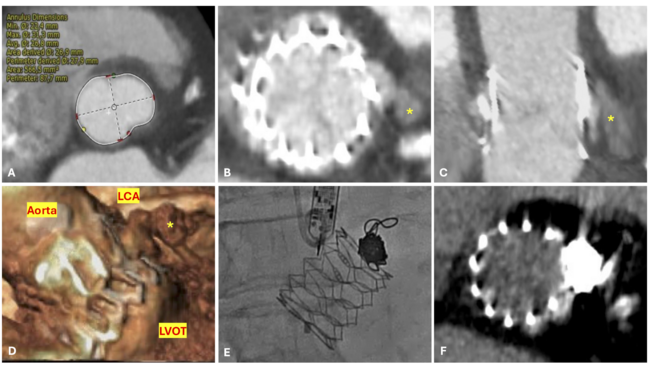
A 64-year-old woman with surgical aortic valve replacement (AVR) using a Mitroflow bioprosthesis (LivaNova) 9 years prior presented with prosthetic valve dysfunction. Because of elevated surgical risk, she underwent valve-in-valve transcatheter aortic valve implantation with a 23-mm Evolut valve (Medtronic). Preprocedural imaging demonstrated high risk of obstruction of the left main (LMCA) and right coronary (RCA) arteries; therefore, chimney stenting was performed with 2 drug-eluting stents (Figure 1, Video 1).
Six months later, the patient developed exertional angina. Coronary angiography (CAG) demonstrated patent chimney stents, and prosthetic valve dysfunction with a maximum transprosthetic gradient of 130 mm Hg was documented. Despite the elevated surgical risk and the presence of chimney stents, the heart team recommended redo surgical AVR.
Both chimney stents were removed, the aortic root was enlarged with a Dacron patch, and a 23-mm St. Jude mechanical prosthesis (Abbott) was implanted. During reconstruction of the RCA ostium, iatrogenic dissection occurred, requiring emergent coronary artery bypass grafting with a saphenous vein graft (SVG) to the posterior descending artery.
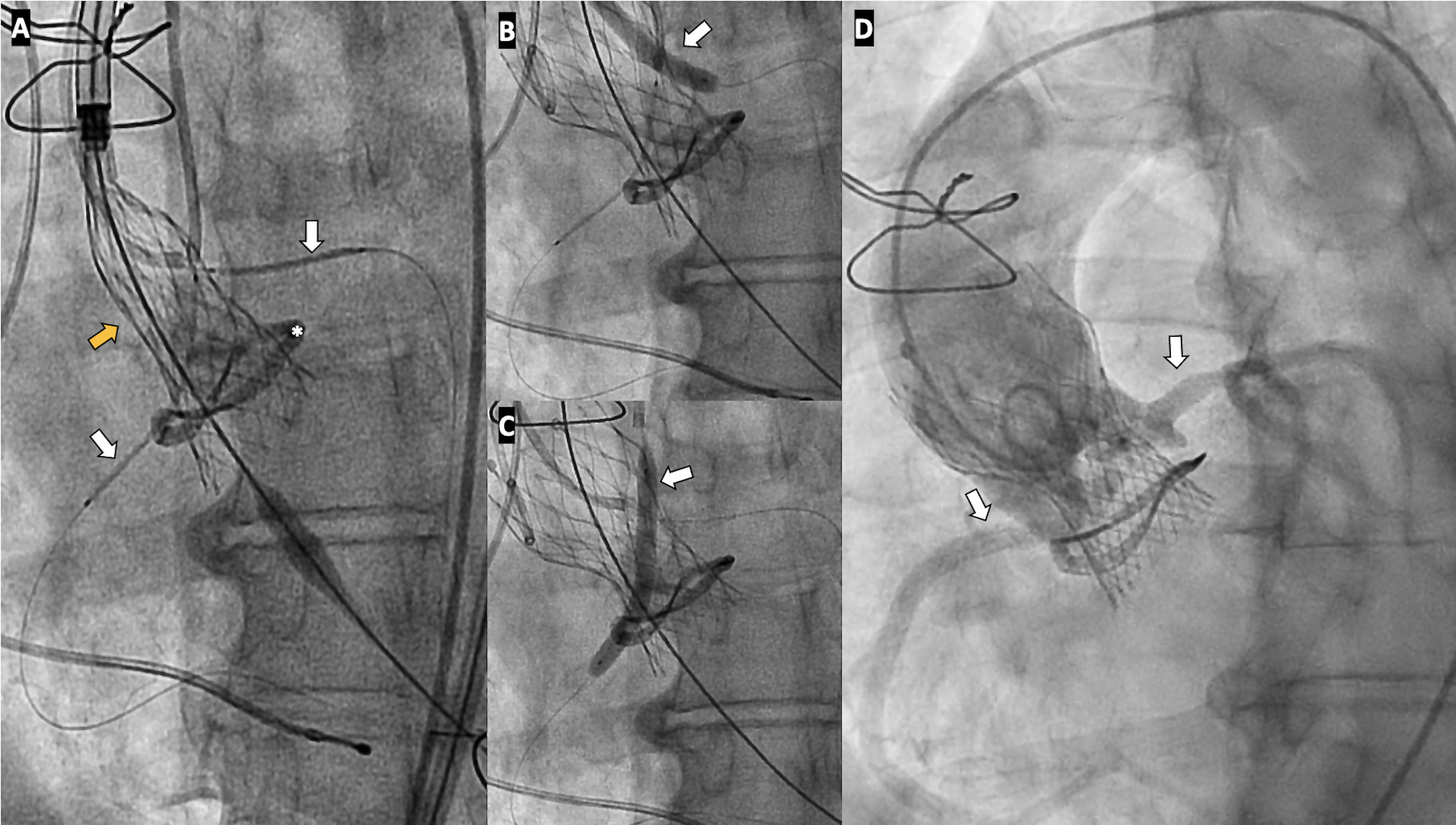
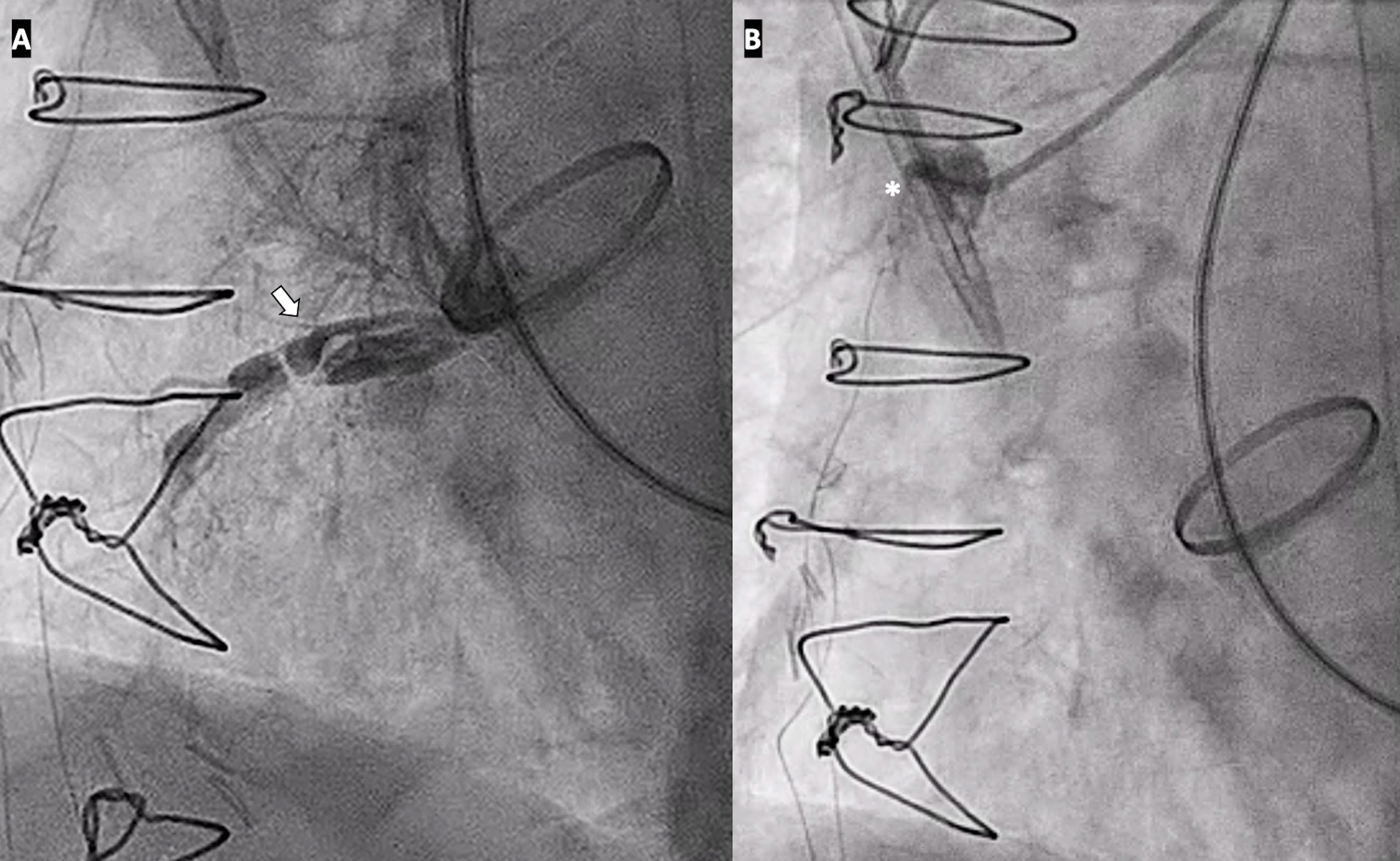
The postoperative course was complicated by cardiogenic shock that required central veno-arterial extracorporeal membrane oxygenation. CAG demonstrated preserved LMCA (Video 2) and extensive RCA ostial dissection with SVG occlusion (Figure 2, Videos 3 and 4). Because of progressive multiorgan failure, conservative management was pursued and the patient died 10 days later.
This case highlights the technical challenges and potential catastrophic complications associated with surgical explantation of coronary chimney stents.
Affiliations and Disclosures
Paula Vela Martín, MD1; Kristian Rivera, MD1,2; Laura Esteban Lucía, MD3; Juan Francisco Oteo Domínguez, MD4
From the 1Department of Cardiology, Arnau de Vilanova University Hospital, Lleida, Spain; 2Grup de Fisiologia i Patologia Cardíaca, Institut de Recerca Biomèdica de Lleida Fundació Dr. Pifarré, IRBLleida, Lleida, Spain; 3Department of Cardiology, General University Hospital, Ciudad Real, Spain; 4Department of Cardiology, Puerta de Hierro Majadahonda University Hospital, Madrid, Spain.
Disclosures: The authors report that they have no financial relationships or conflicts of interest with respect to the content herein.
Ethics statement: This article was carried out in accordance with the local ethics committee regulations and the Code of Ethics of the World Medical Association (Declaration of Helsinki) for experiments involving humans. Written informed consent for publication was obtained from the patient’s family.
Address for correspondence: Paula Vela Martín, MD, Arnau de Vilanova University Hospital, Av. Rovira Roure 80, Lleida 25198, Spain. Email: pvela.lleida.ics@gencat.cat