

Resistant Hypertension Due to Renal Artery Stenosis in Neurofibromatosis Type 1: Successful Management With Stenting
© 2025 HMP Global. All Rights Reserved.
Any views and opinions expressed are those of the author(s) and/or participants and do not necessarily reflect the views, policy, or position of the Journal of Invasive Cardiology or HMP Global, their employees, and affiliates.
A 52-year-old man with a known history of neurofibromatosis type 1 (NF-1) was referred to our clinic for evaluation of resistant hypertension. The patient was on 4 antihypertensives at baseline: amlodipine 10 mg once daily, combination of telmisartan 40 mg and hydrochlorthiazide 12.5 mg once daily, and bisoprolol 2.5 mg once daily. Because he did not have adequate blood pressure (BP) control despite the use of adequate doses of more than 3 antihypertensive agents including a diuretic, he was labelled as a case of resistant hypertension and referred to us for further management.
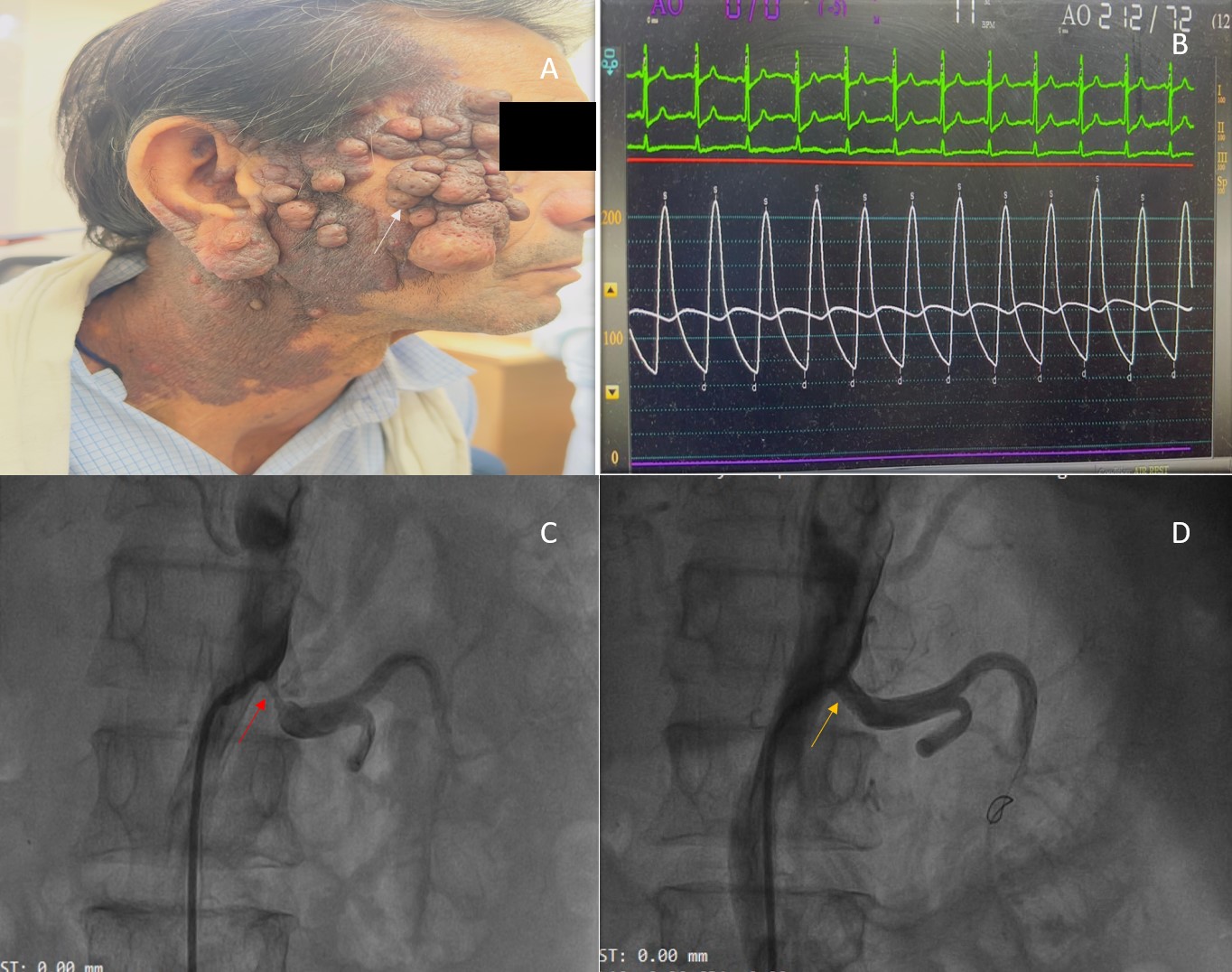
On examination, his BP was 220/100 mm Hg and his heart rate was 90 beats per minute. Multiple cutaneous neurofibromas and areas of hyperpigmentation were noted over his face and neck (Figure A). Electrocardiography demonstrated normal sinus rhythm with evidence of left ventricular hypertrophy. Transthoracic echocardiography revealed concentric left ventricular hypertrophy with preserved systolic function, without evidence of aortic coarctation or stenosis. Laboratory investigations showed elevated serum creatinine (1.7 mg/dL; normal 0.6-1.1 mg/dL).
The most common vascular abnormality in NF-1 is unilateral or bilateral renal artery stenosis.1 Careful examination revealed a left-sided renal vascular bruit. Renal artery Doppler study suggested significant left renal artery stenosis, which was confirmed on computed tomography angiography. After multidisciplinary discussion, revascularization of the left renal artery was planned.
In the catheterization laboratory, the patient’s invasive BP measured 212/72 mm Hg (Figure B). The right renal artery had a mild plaque at the ostium and was free of significant disease. Left renal angiography demonstrated 90% proximal stenosis of the left renal artery (Figure C). The lesion was crossed with a Whisper wire (Abbott), followed by predilatation using a 4 ×18-mm Apollo balloon (BrosMed Medical). A 7×18-mm Herculink Elite stent (Abbott) was then deployed. Postdilatation with a noncompliant balloon and ostial flaring were performed, resulting in a well-expanded stent with satisfactory distal flow (Figure D).
The patient was not initiated on any new medications following the procedure. Prior to intervention, he had been on 4 antihypertensive agents with inadequate BP control. After the procedure, his regimen was reduced to amlodipine 5 mg once daily and bisoprolol 2.5 mg once daily. The effective control of BP on lower doses of just 2 agents, in contrast to poor control with 4 drugs pre-procedure, strongly supports that stenting and relief of renal artery stenosis played a pivotal role in achieving adequate BP control. At the 8-month follow-up, the patient was doing well on 2 antihypertensive agents with a BP of 130/70 mm Hg and normalization of serum creatinine.
This case highlights the strong association of NF-1 with renal artery stenosis. A high index of suspicion is essential for timely diagnosis in patients presenting with resistant hypertension, as prompt revascularization can significantly improve outcomes.2
Affiliations and Disclosures
Saurabh Kumar Singh, MD, DM1; Devesh Kumar, MD, DM1; Shrividya Rao, MS, MCH2; Shilpi Rani, MD1; Krishna Prasad Akkineni, MD, DM3
From the 1Department of Cardiology, Safdarjung Hospital, New Delhi, India; 2Department of Cardiothoracic and Vascular Surgery, All India Institute of Medical Sciences, New Delhi, India; 3Department of Cardiology, Apollo Hospitals, Jubilee Hills, Hyderabad, India.
Disclosures: The authors report no financial relationships or conflicts of interest regarding the content herein.
Consent statement: The authors confirm that informed consent was obtained from the patient for the intervention described in the manuscript and for the publication thereof, including photographs.
Address for correspondence: Krishna Prasad Akkineni, MD, DM, Room number 1, Ground floor, Apollo Hospitals, Jubilee Hills, Hyderabad 500033, India. Email: ramuchinnu92@gmail.com; Instagram: @krishnaakkineni
References
- Duan L, Feng K, Tong A, Liang Z. Renal artery stenosis due to neurofibromatosis type 1: case report and literature review. Eur J Med Res. 2014;19(1):17. doi:10.1186/2047-783X-19-17
- Malav IC, Kothari SS. Renal artery stenosis due to neurofibromatosis. Ann Pediatr Cardiol. 2009;2(2):167-169. doi:10.4103/0974-2069.58323










