


Imaging Insights Into Endothelial Response: Cardiac Computed Tomography Assessment of WATCHMAN FLX and FLX Pro
© 2026 HMP Global. All Rights Reserved.
Any views and opinions expressed are those of the author(s) and/or participants and do not necessarily reflect the views, policy, or position of the Journal of Invasive Cardiology or HMP Global, their employees, and affiliates.
J INVASIVE CARDIOL 2026. doi:10.25270/jic/26.00003. Epub May 29, 2026.
Abstract
Objectives. Hypoattenuated thickening (HAT) on cardiac computed tomography (CT) is recognized as a marker of thrombotic risk following left atrial appendage occlusion (LAAO). The WATCHMAN FLX Pro (Boston Scientific) introduces design changes to improve sealing and endothelialization, yet its impact on HAT remains unknown. The authors conducted a comparative CT-based evaluation of the WATCHMAN FLX and FLX Pro to assess early endothelial response and device performance.
Methods. The authors reviewed the 4-month follow-up cardiac CT of 214 patients who underwent LAAO at a single institution (133 with FLX, 81 with FLX Pro). Scans were blindly reviewed for presence, morphology, and thickness of HAT, appendage patency, and peridevice leak.
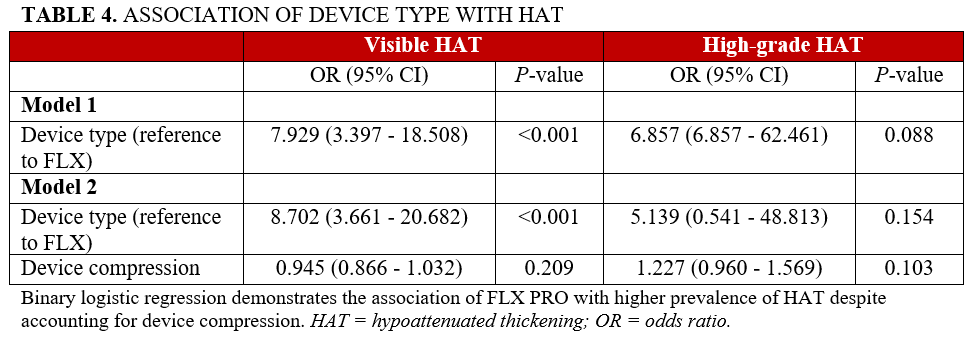
Results. Patient characteristics were similar across groups except for higher HAS-BLED scores and greater device compression in FLX Pro recipients. Visible HAT was significantly more prevalent in FLX Pro patients (91.4% vs 57.1%; odds radio [OR]: 8.702 [95% CI, 3.661-20.682]; P < .001), with greater total HAT thickness (3.2 vs 1.7 mm, P < .001). High-grade HAT was numerically more frequent in the FLX Pro group (4.9% vs 0.8%, P = .069). Incomplete endothelium formation (appendage patency without peridevice leak) was less common with FLX Pro (3.7% vs 15.8%; OR: 0.244 [95% CI, 0.069-0.857]; P = .028).
Conclusions. This is the first comparative CT-based analysis of the WATCHMAN FLX and FLX Pro. There was improved appendage sealing as evidenced by decreased appendage patency without peridevice leak with the FLX Pro device. Additionally, HAT was more frequently visible with the newer generation device and presented with thicker and more pronounced phenotypes.
Introduction
Left atrial appendage occlusion (LAAO) is an increasingly utilized alternative to long-term oral anticoagulation (OAC) for stroke prevention in patients with atrial fibrillation (AFIB) who have contraindications to systemic therapy. The WATCHMAN family of devices (Boston Scientific) has emerged as the most widely adopted LAAO platform in the United States.
Postprocedural surveillance is evolving toward cardiac computed tomography (CT), which offers superior spatial resolution for assessing device position, appendage patency/sealing, peridevice leak (PDL), and early healing.1-4 There is growing interest in hypoattenuated thickening (HAT), seen on CT along the face of the device. Prior studies have characterized HAT as a spectrum—ranging from thin, smooth, low-grade coverage to thick, irregular, high-grade formations that may correspond to device-related thrombus (DRT).5 The latter HAT morphologies raise concerns about being a risk factor for thromboembolic events and often prompt intensification of antithrombotic therapy.
The recently introduced WATCHMAN FLX Pro incorporates a fluoropolymer—expanded polytetrafluoroethylene (ePTFE)—coating over its fabric cap to improve sealing and accelerate endothelialization.6 However, its impact on early healing patterns and device sealing in humans remains unknown. It remains unclear whether the FLX Pro alters the prevalence, thickness, or morphology of HAT, and how these findings should guide post-implant antithrombotic therapy. No study to date has systematically characterized HAT after FLX Pro implantation using standardized CT protocols.
We sought to address this knowledge gap by performing the first comparative CT-based evaluation of HAT between the WATCHMAN FLX Pro device and its predecessor, the WATCHMAN FLX. Our aim was to determine whether the FLX Pro’s design modifications influence early healing, to describe any unique morphologic patterns, and to explore potential implications for post-LAAO surveillance and management.
Methods
Study population
We retrospectively identified consecutive patients who underwent successful LAAO with either the WATCHMAN FLX or WATCHMAN FLX Pro device at our institution between 2022 and 2024. These patients had been referred for LAAO because of a prior history of significant bleeding and/or a demonstrated difficulty with OAC administration. Implantation was pursued after independent agreement amongst 2 cardiologists regarding candidacy for LAAO. Patients underwent implantation with the FLX prior to July of 2024 and, subsequently, our institution switched to the FLX Pro. Patients were eligible for inclusion if they underwent standardized follow-up cardiac CT at approximately 4 months post-procedure. Exclusion criteria included technically inadequate CT studies (eg, motion artifact, incomplete coverage) or absence of follow-up imaging within the prespecified time window.
Procedural details
All patients underwent a preprocedural echocardiogram to evaluate existing pericardial effusion and a preprocedural CT to evaluate the presence of LAA thrombus, trans-septal planning, and preliminary device sizing. Size selection was based on 15% to 25% device compression as predicted by the TruPlan software system (Circle CVI). All procedures were performed under moderate sedation via transfemoral venous access with transseptal puncture using the VersaCross system (Baylis Medical) and under intracardiac echocardiography using an 8F ACUSON AcuNav probe (Siemens Healthineers) and fluoroscopic guidance. Device deployment followed manufacturer instructions and satisfaction of the PASS (Position, Anchor, Size, Seal) criteria. Device compression was calculated as:

A postprocedural echocardiogram was done following the procedure to confirm absence of significant pericardial effusion, and most patients underwent same-day discharge. All patients were placed on dual antiplatelet therapy (DAPT) with aspirin and a P2Y12 inhibitor for 6 months followed by aspirin monotherapy. No patients were treated with OAC therapy after device implantation.
Cardiac CT acquisition and analysis
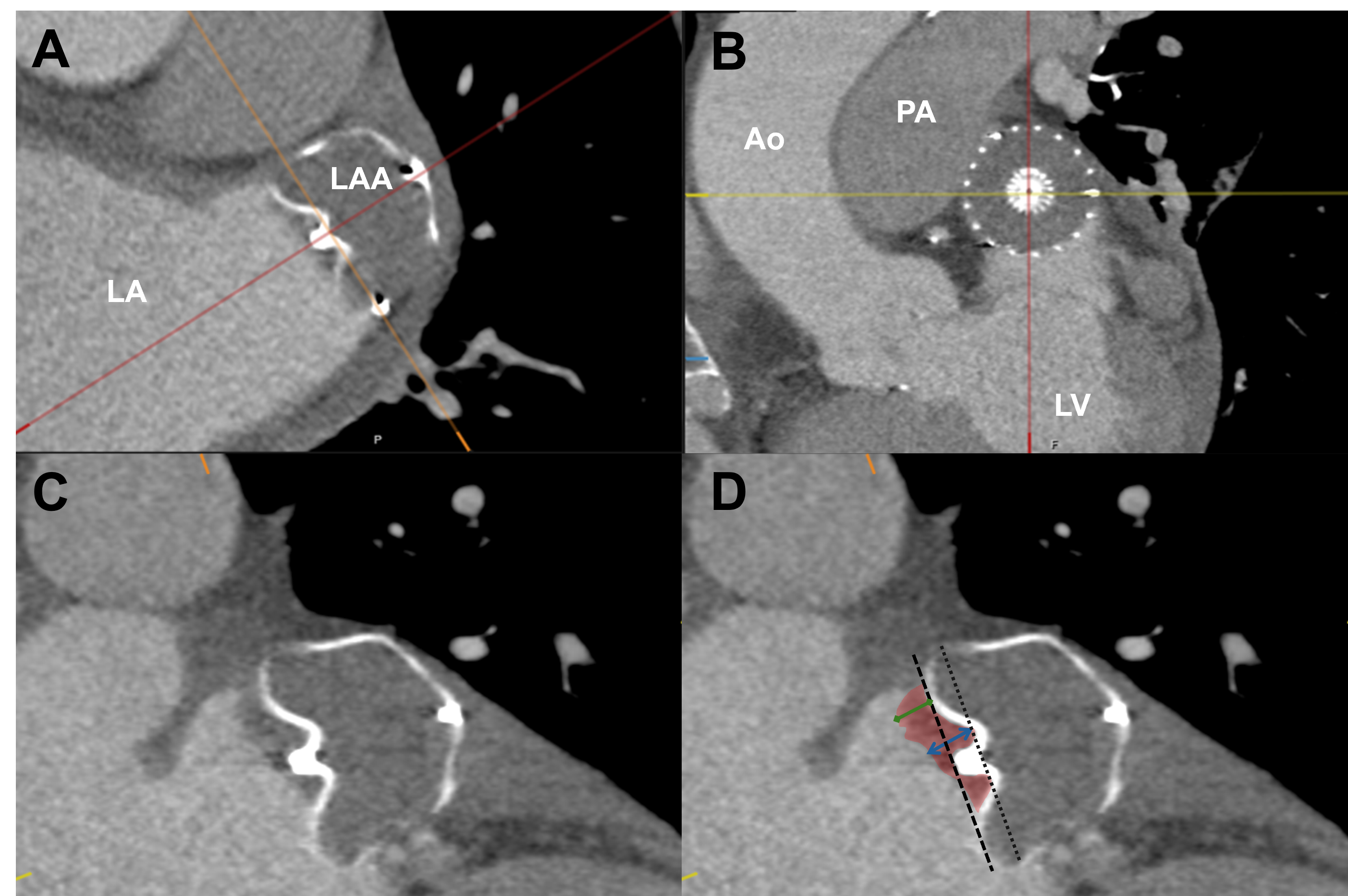
All patients underwent contrast-enhanced, prospective electrocardiogram-gated cardiac CT (128 x 0.6-mm, dual-source [Siemens Heathineers]) at approximately 4 months post-implant with a standardized LAAO protocol (scanned first rib to diaphragm after 5 cc/sec for 80 cc extended contrast bolus).7 Images were blindly analyzed at 35% of the cardiac cycle. Using multiplanar reconstruction, en face views of the implanted WATCHMAN device were created by centering the crosshair on the device screw and aligning orthogonal planes with the screw and through the device shoulders at the level of the screw hub cove, as previously described (Figure 1A and B).5 HAT was defined as hypoattenuation visualized from the atrial side to the bottom of the screw hub cove (Figure 1C and D). Superficial HAT was defined as the hypoattenuation present from the atrial side to the proximal part of the device frame, excluding the screw hub cove, as previously described (Figure 1D).5
Each scan was assessed for the following:
- LA area (mm2)
- Presence of HAT/superficial HAT (yes/no)
- HAT/superficial HAT thickness (mm)
- HAT/superficial HAT Area (mm2)
- HAT morphology (smooth, irregular, pedunculated, continuity with the LA wall)
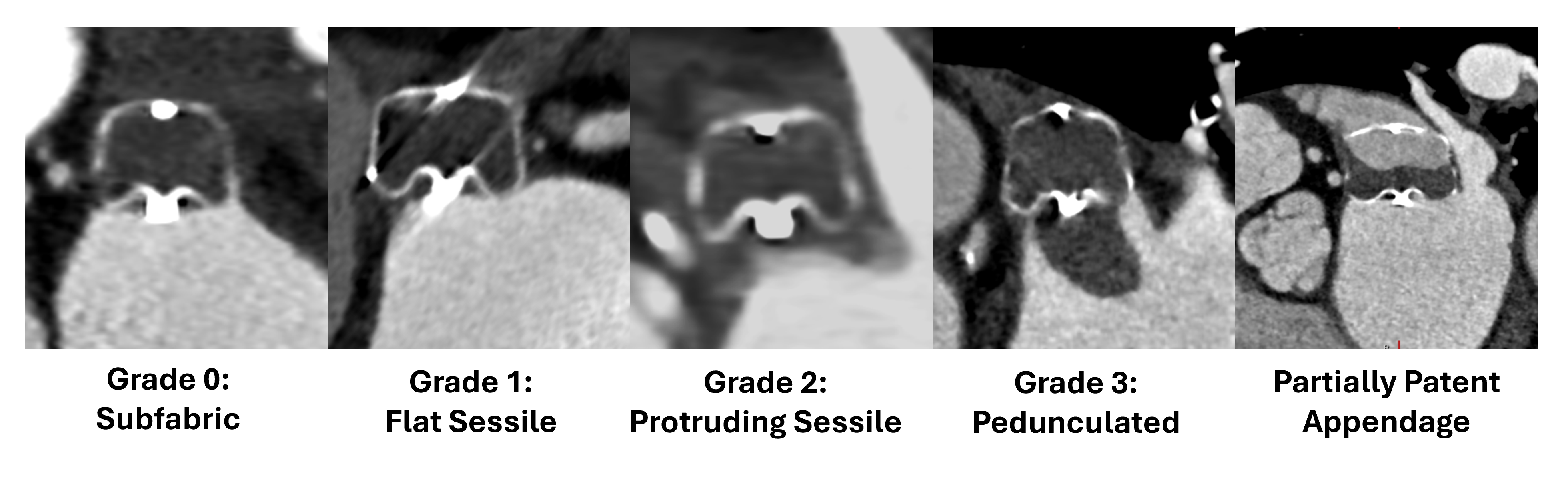
- HAT grading (as previously described)5
- Grade 0: Subfabric – Unappreciable HAT or HAT present in the screw hub cove below the proximal frame of the device
- Grade 1: Flat sessile – HAT extending beyond the proximal frame but ≤3 mm in thickness
- Grade 2: Protruding sessile – HAT extending beyond the proximal frame and >3 mm in thickness
- Grade 3: Pedunculated – Asymmetric, irregular, and >3 mm in thickness
- Appendage patency (contrast opacification of the LAA beyond the device face, yes/no)
- Peridevice leak – (yes/no and width)
- Device depth (mm)
Grades 2 and 3 HAT were considered high-grade. A patent appendage without concomitant PDL was deemed representative of incomplete endothelium formation.8
Outcomes
The primary endpoint was prevalence of high-grade HAT on follow-up CT. Secondary endpoints included prevalence of HAT, HAT/superficial HAT thickness/area, appendage patency without leak, and peridevice leak.
Statistical analysis
Continuous variables are presented as mean ± standard deviation and compared using the Mann-Whitney U test between the 2 independent groups. Categorical variables are expressed as counts (percentages) and compared using chi-square testing or Fisher’s exact test when expected cell counts were small. Logistic regression was performed to estimate odds ratios (OR) with 95% confidence intervals (CI) for associations between device type and presence of HAT, high-grade HAT, patent LAA, and incomplete endothelium formation. A 2-tailed P-value of less than 0.05 was considered statistically significant. Analyses were performed using SPSS, version 24 (IBM).
Results
Study population
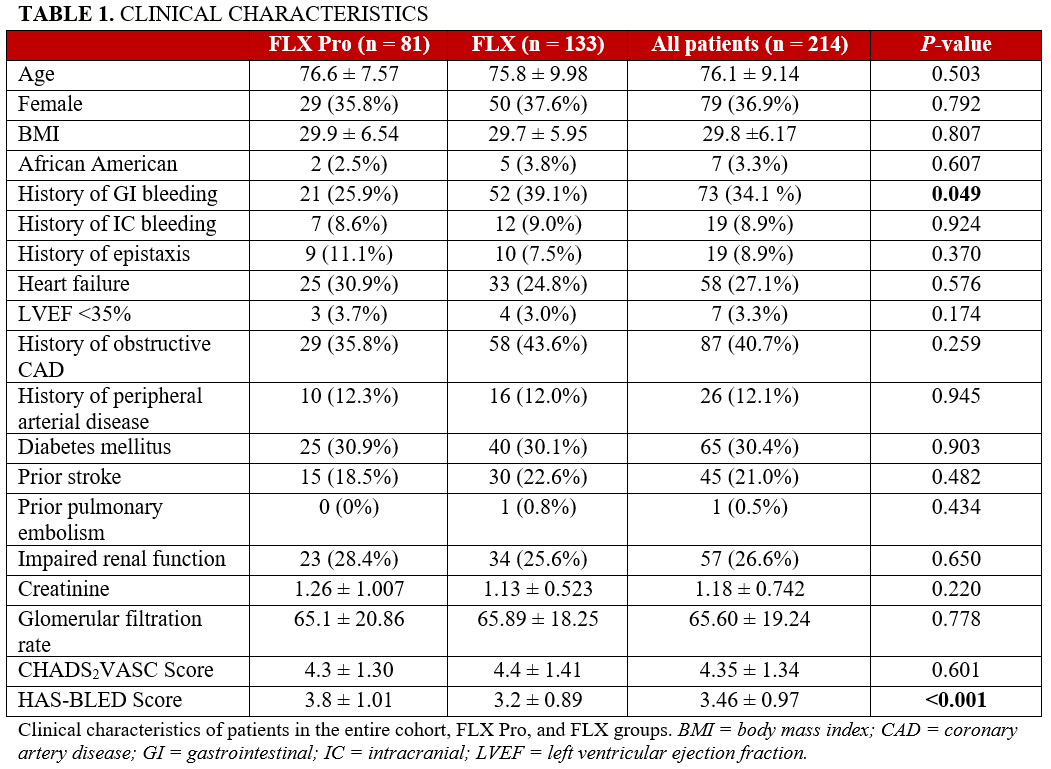
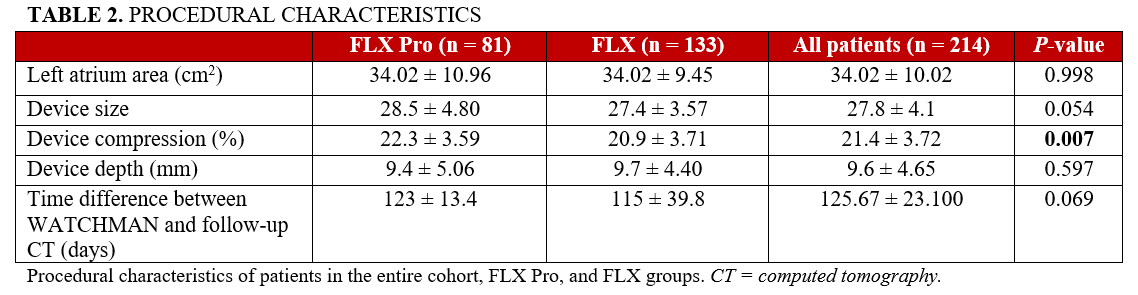
A total of 214 patients met inclusion criteria: 133 received a WATCHMAN FLX and 81 received a WATCHMAN FLX Pro. The mean age was 76.1 ± 9.14 years, and 36.9% were female. Baseline demographic and procedural characteristics were generally similar between groups (Tables 1 and 2), with 2 notable differences: FLX Pro recipients had higher mean HAS-BLED scores (3.8 ± 1.01 vs 3.2 ± 0.89, P < .001) and greater mean device compression at implant (22.3% ± 3.59% vs 20.9% ± 3.71%, P = .007).
HAT
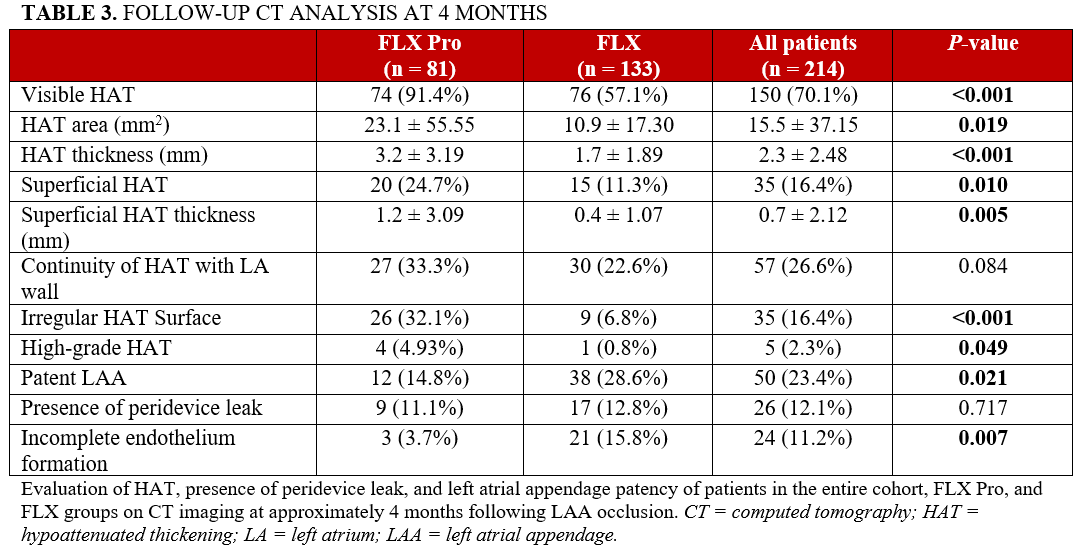
Visible HAT was significantly more prevalent among FLX Pro recipients compared with FLX recipients (91.4% vs 57.1%; OR: 8.702; 95% CI, 3.661-20.682; P < .001) (Tables 3 and 4). Mean HAT thickness was greater in the FLX Pro group (3.2 ± 3.19 mm vs 1.7 ± 1.89 mm, P < .001). Mean HAT area was higher in the FLX Pro group (23.1 ± 55.55 mm2 vs 10.9 ± 17.30 mm2, P = .019). Mean superficial HAT thickness was also greater in the FLX Pro group (1.2 ± 3.09 mm vs 0.4 ± 1.07 mm, P = .005). These results altogether suggest a more prominent HAT following FLX Pro implantation.
HAT morphology and grading
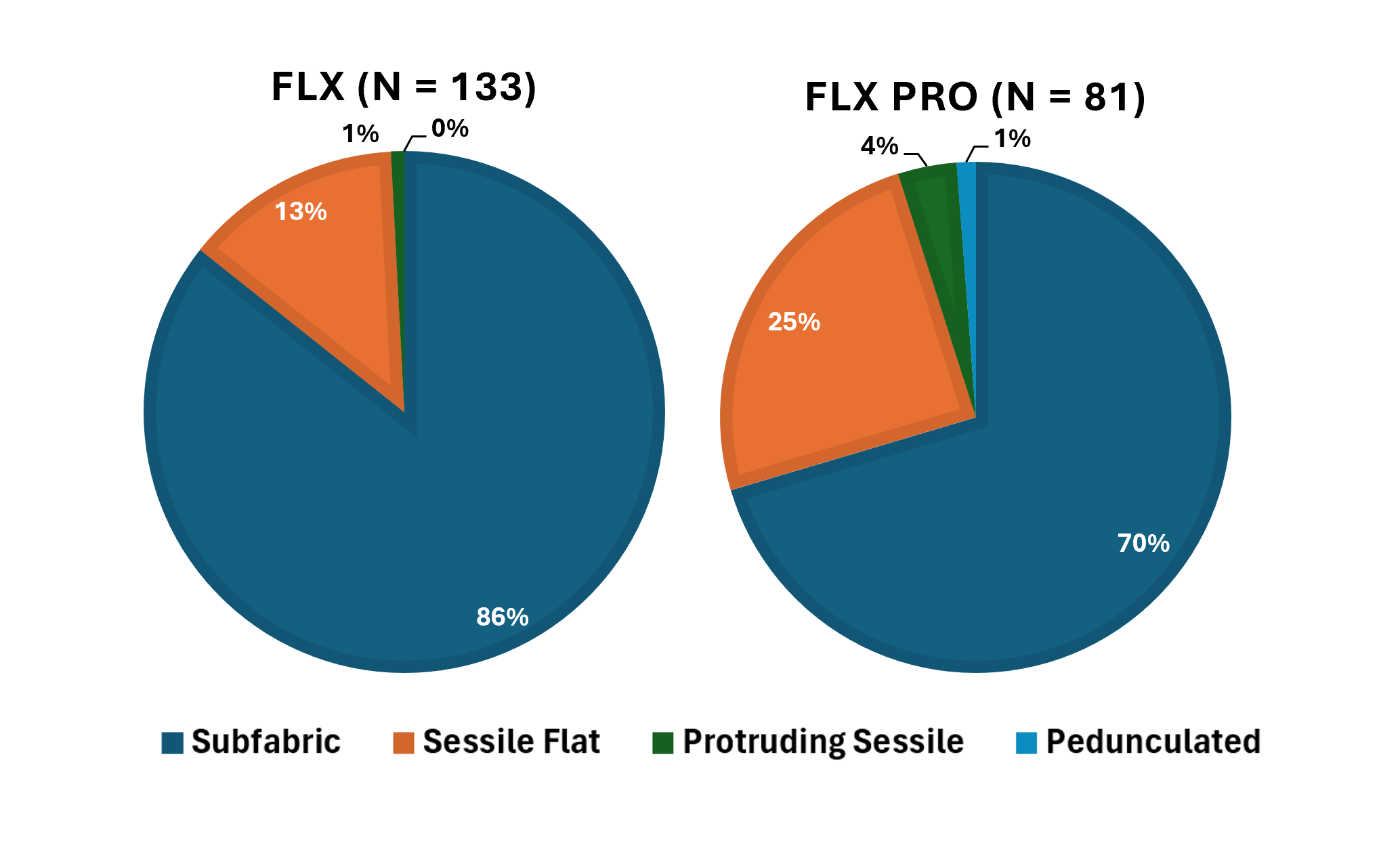
Continuity of HAT with the LA wall did not differ between groups. High-grade HAT occurred in 4.93% of FLX Pro patients vs 0.8% of FLX patients (P = .069). After adjustment for device compression, FLX Pro was not associated with high-grade HAT (adjusted OR: 5.139; 95% CI, 0.541-48.813; P = .154; Table 4). Of the patients with high-grade HAT, 2 (1 FLX Pro and 1 FLX) were not found to have evidence of DRT on transesophageal echocardiography (TEE). One patient (FLX Pro) with Grade 2 HAT experienced ischemic stroke within 4 months of follow-up. Representative low- and high-grade HAT appearances are shown in Figure 2, and grade distribution by device type in Figure 3. High-grade HAT was more prevalent in patients with deeper devices (19.1 ± 8.69 vs 9.3 ± 4.30 mm, P < .001) and a left ventricular ejection fraction of less than 35% (20.0% vs 2.9%, P = .033), though these characteristics were similar between the 2 device groups.
Appendage patency and peridevice leak
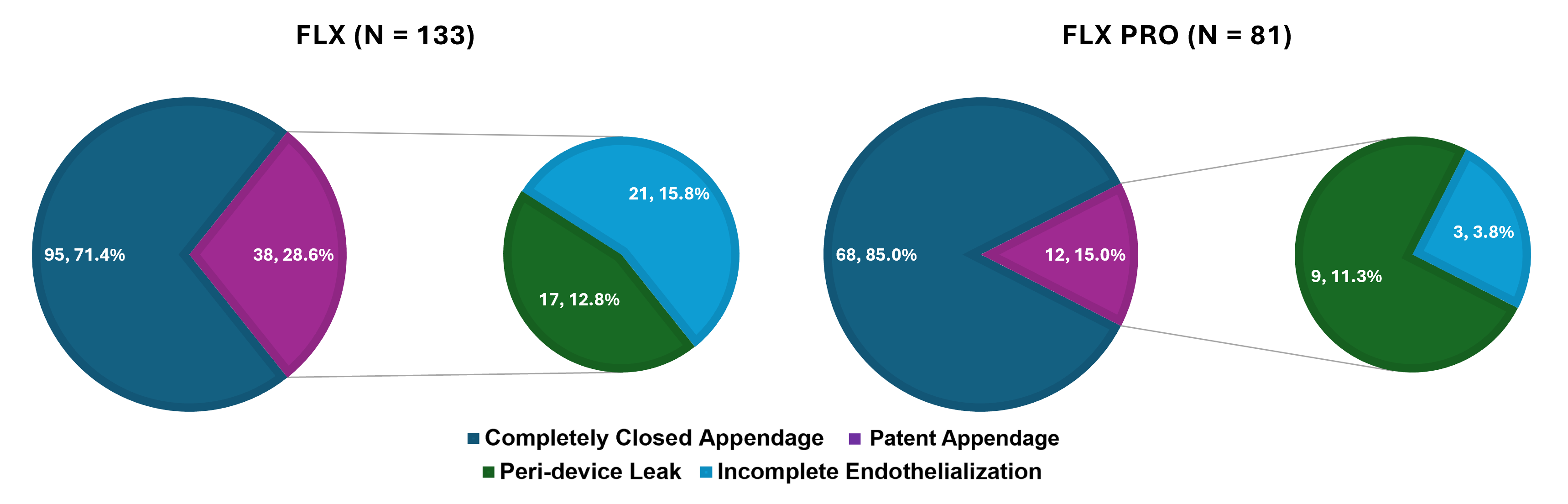
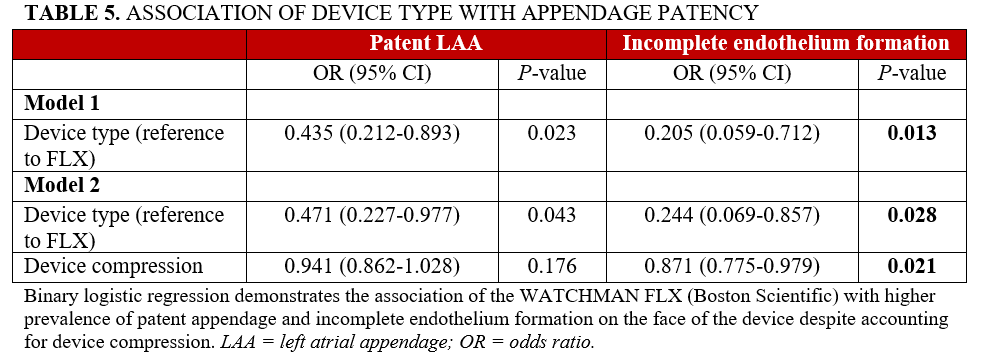
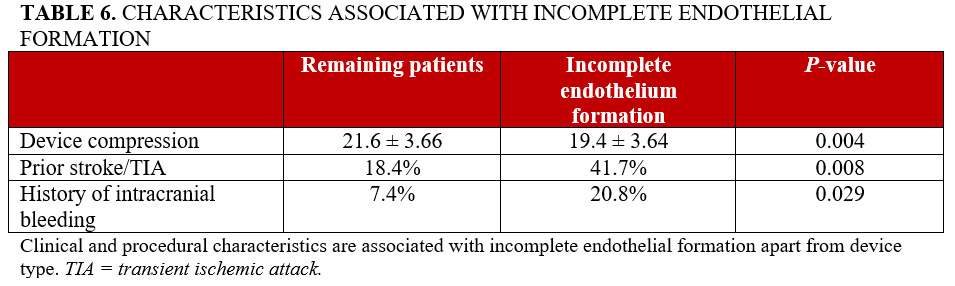
At follow-up CT, appendage patency was more frequently observed in the FLX group compared with the FLX Pro group (28.6% vs 14.8%, P = .021 (Table 3, Figure 4). Among patients with patent appendages, almost half had peridevice leak (PDL), with no significant difference in PDL prevalence between device types. The remainder—appendage patency without leak—was presumed to represent incomplete endothelial coverage. This finding was significantly less frequent with the FLX Pro after adjustment for device compression (adjusted OR: 0.244; 95% CI, 0.069-0.857; P = .028) (Table 5). Other factors that were associated with incomplete endothelium formation include device compression, history of prior stroke/transient ischemic attack, and history of intracranial bleeding (Table 6) though these factors were not significantly different between the 2 device cohorts.
Discussion
In this comparative, CT-based analysis of 214 real-world LAAO recipients, WATCHMAN FLX Pro implantation was associated with more pronounced HAT and reduced patent appendages without PDL at 4 months compared with the WATCHMAN FLX. The signal for HAT was consistent across multiple metrics—prevalence, thickness, area, and morphologic complexity—suggesting an intrinsic device-related effect. Notably, high-grade HAT (the morphology most often considered worrisome for DRT) was numerically higher in the FLX Pro group, but regression analysis did not demonstrate a clear association with device type and high-grade HAT. These findings are likely associated with the ePTFE coating on the newer generation device and have important implications for imaging surveillance and post-implant management.
Our findings with the FLX group are remarkably consistent with prior CT-based WATCHMAN FLX studies, which report a HAT prevalence of 64%, high-grade HAT in fewer than 3% of patients, patent appendages in 31.7% of cases, and 11.5% of subjects having patent appendages without PDL.5 In contrast, the FLX Pro cohort in this study demonstrated a HAT prevalence of greater than 90%. However, the prevalence of high-grade HAT in the FLX Pro group was still low (4.93%), with 1 patient not having any evidence of DRT on TEE.
This high-grade HAT burden is relatively consistent with prior TEE- and CT-based studies with the FLX device, which report DRT rates of 3% to 4%.9-10 Moreover, patent LAAs were seen half as frequently with our FLX Pro cohort, with a greater than 4-fold decrease in patent LAAs without PDL compared with the FLX group. As such, our results illustrate a distinct healing phenotype with the newer generation device without a clear suggestion for greater DRT. It is noteworthy that, in earlier FLX studies, HAT thickness and morphology tended to improve over time, with high-grade lesions often resolving under intensified antithrombotic therapy.1-5 No comparable temporal data exist for FLX Pro. Whether our findings reflect a transient, polymer-related healing phenotype or a more persistent thrombotic tendency remains unknown. Ongoing studies, including the FLX Pro CT Pilot, are expected to provide important insights into the temporal evolution of device healing with serial imaging.11
The FLX Pro incorporates a poly (vinylidene fluoride-co-hexafluoropropylene) (PVDF-HFP) fluoropolymer coating on its atrial surface called HEMOCOAT. This non-eluting polymer is expected to be hemocompatible and promote faster endothelium formation. In-vitro studies demonstrated this polymer coating to have increased albumin binding and decreased platelet adhesion after exposure to human blood.6 Implantation of the coated device in non-anticoagulated canines was associated with less thrombogenicity at 14, 28, and 45 days as assessed by TEE and improved neo-endocardial formation at 45 days compared with controls at necropsy. Enhanced endothelial coverage was also seen in a porcine model at 90 days post-implantation of the coated device, but complete endothelial coverage was also present with the uncoated device.6 Our human imaging data appears to be reflective of the enhanced endothelial coverage seen in the aforementioned animal testing. FLX Pro recipients exhibited more extensive HAT and fewer cases of appendage patency without peridevice leak—suggesting improved endothelial formation from the fluoropolymer coating.
One plausible mechanism is that the surface chemistry of PVDF-HFP alters the initial healing trajectory. The coating on the FLX Pro device may influence fibrin deposition, leading to denser or more persistent fibrin structures. Furthermore, the polymer’s surface properties potentially accelerate early endothelial cell migration, facilitating a more robust neo-endothelial layer and improved appendage sealing that yields more pronounced HAT and decreased appendage patency on CT. Given that neoendothelialization is a time-dependent process,5,12 the single approximately 4-month CT snapshot may capture the FLX Pro device during this transient, bulkiest healing phase, while the uncoated FLX might have already progressed to a more stable state. As such, an increase in CT-visible HAT may not therefore necessarily equate to a proportional increase in embolic risk. However, the more pronounced HAT in the FLX Pro group is clinically noteworthy for post-procedure surveillance, as high-grade patterns typically raise concern for embolic events.13-14 Further studies are needed to assess whether the increased HAT and decrease in appendage patency seen with FLX Pro is associated with a change in embolic risk.
Additionally, our findings may be a consequence of the post-implantation antithrombotic regimen. While there is substantial variation in antithrombotic regimens post LAAO—which may have significant implications of HAT phenotype and DRT prevalence—all patients in our study received DAPT with aspirin and a P2Y12 inhibitor for 6 months followed by aspirin monotherapy, thereby removing postprocedural antithrombotic therapy as a confounder. Notably, results from the SURPASS Pro multicenter registry demonstrate only a slightly higher incidence of DRT with the FLX Pro compared with the earlier generation device (0.5% vs 0.4%) without a greater prevalence of ischemic stroke (0.1% vs 0.2%).15 However, in contrast to our study, the majority of patients in SURPASS Pro were discharged on a direct oral anticoagulant (DOAC) with only 37% of patients given DAPT following LAAO. Thereby, it is possible that the more pronounced HAT seen with the FLX Pro in our cohort is associated with our DAPT regimen. In fact, a single center study of 130 patients with FLX Pro demonstrated an elevated risk of DRT without thromboembolism in patients receiving DAPT (compared with DOAC) following FLX Pro implantation, with resolution of DRT following a transition to DOAC therapy.16 Collectively, these results raise concern for an increased risk of high-grade HAT/DRT following FLX Pro implantation and DAPT therapy. The highly anticipated SIMPLAAFY trial is expected to further clarify the optimal antithrombotic regimen.
Limitations
Our study should be interpreted within the constraints of its retrospective, single-center design. The small sample size limits subgroup analyses. Imaging was performed only at a single time point (~4 months), so the temporal evolution of HAT with FLX Pro remains unknown. Additionally, within the high-grade HAT subgroup, only 1 stroke event was observed, precluding any meaningful assessment of the relationship between HAT phenotype and thromboembolic risk.
Conclusions
This is, to our knowledge, the first human imaging study to compare CT findings between WATCHMAN FLX and FLX Pro devices. The FLX Pro device was associated with a higher prevalence of visible HAT, and all quantitative markers of HAT were greater in the FLX Pro group. The finding of more pronounced HAT with the polymer-coated device with improved appendage sealing highlights a significant difference in healing biology that has important implications regarding postprocedural surveillance and the design of future device iterations, and merits longitudinal investigation.
Affiliations and Disclosures
Rafey Feroze, MD1; Marco Frazzetto, MD2; Luis Augusto Palma Dallan, MD, PhD1; Mohammed Alghammass, MD1; Yusef Saeed, MD3; Maedeh Z. Nikoo, MD3; Alexander Cove, MD3; Nawaf Alhabdan, MD3; Abdullah Altorbag, MD3; Andreas A. Towers, MD3; Steven J. Filby, MD1
From the 1Division of Cardiology, University Hospitals, Cleveland, Ohio; 2Cardiocentro Ticino Institute, Lugano, Switzerland; 3Division of Internal Medicine, University Hospitals, Cleveland, Ohio.
Disclosures: Dr Filby is a consultant for Boston Scientific. The remaining authors report no financial relationships or conflicts of interest regarding the content herein.
Address for correspondence: Steven J. Filby, MD, 11100 Euclid Avenue, Cleveland, OH 44106, USA. Email: Steven.Filby@UHHospitals.org
References
1. Tiroke LH, Kramer A, Poulsen MW, et al. Long-term cardiac computed tomography follow-up after left atrial appendage occlusion. EuroIntervention. 2024;20(11):e718-e727. doi:10.4244/EIJ-D-23-00802
2. Korsholm K, Iriart X, Saw J, et al. Position statement on cardiac computed tomography following left atrial appendage occlusion. JACC Cardiovasc Interv. 2024;17(15):1747-1764. doi:10.1016/j.jcin.2024.04.050
3. Yoon SH, Amoah JK, Galo J, et al. Incidence, progression, and predictors of left atrial appendage sealing after Watchman FLX device implantation with computed tomographic assessment. Catheter Cardiovasc Interv. 2024;103(6):995-1003. doi:10.1002/ccd.31044
4. Tan BE, Baqai F, Padilla F, et al. Cardiac CT versus transesophageal echocardiography following left atrial appendage closure: a systematic review and meta-analysis. Circ Cardiovasc Imaging. 2025;18(8):e018151. doi:10.1161/CIRCIMAGING.125.018151
5. Kramer AD, Korsholm K, Jensen J, et al. Cardiac computed tomography following Watchman FLX implantation: device-related thrombus or device healing? Eur Heart J Cardiovasc Imaging. 2023;24(2):250-259. doi:10.1093/ehjci/jeac222
6. Saliba WI, Kawai K, Sato Y, et al. Enhanced thromboresistance and endothelialization of a novel fluoropolymer-coated left atrial appendage closure device. JACC Clin Electrophysiol. 2023;9(8 Pt 2):1555-1567. doi:10.1016/j.jacep.2023.04.013
7. Kuroki K, Doshi SK, Whang W, et al. Follow-up imaging after left atrial appendage closure. Heart Rhythm. 2020;17(11):1848-1855. doi:10.1016/j.hrthm.2020.06.024
8. Sivasambu B, Arbab-Zadeh A, Hays A, Calkins H, Berger RD. Delayed endothelialization of watchman device identified with cardiac CT. J Cardiovasc Electrophysiol. 2019;30(8):1319-1324. doi:10.1111/jce.14053
9. Sakriss C, Roehl P, Schwenzky A, Hoyme M, Ebelt H. Transition from WATCHMAN V.2.5 to WATCHMAN FLX for closure of the left atrial appendage: echocardiographic and clinical findings. Open Heart. 2023;10(1):e002246. doi:10.1136/openhrt-2022-002246.
10. Galea R, Mahmoudi K, Gräni C, et al. Watchman FLX vs. Watchman 2.5 in a Dual-Center Left Atrial Appendage Closure Cohort: the WATCH-DUAL study. Europace. 2022;24(9):1441-1450. doi:10.1093/europace/euac021
11. WATCHMAN FLX Pro CT pilot study. ClinicalTrials.gov identifier: NCT05567172. Updated December 9, 2025. Accessed January 22, 2026. https://clinicaltrials.gov/study/NCT05567172?term=NCT05567172&rank=1
12. Akinapelli A, Bansal O, Chen JP, et al. Left atrial appendage closure -the WATCHMAN device. Curr Cardiol Rev. 2015;11(4):334-340. doi:10.2174/1573403X11666150805115822
13. Simard T, Jung RG, Lehenbauer K, et al. Predictors of device-related thrombus following percutaneous left atrial appendage occlusion. J Am Coll Cardiol. 2021;78(4):297-313. doi:10.1016/j.jacc.2021.04.098
14. Iriart X, Blanc G, Bouteiller X, et al. Clinical implications of CT-detected hypoattenuation thickening on left atrial appendage occlusion devices. Radiology. 2023;308(3):e230462. doi:10.1148/radiol.230462
15. Piccini JP, Zeitler EP, Yeh R, et al. PO-02-184 Outcomes with Watchman FLX PRO in everyday clinical practice: early results from SURPASS PRO. Heart Rhythm. 2025;22(4):S318. doi:10.1016/j.hrthm.2025.03.666
16. Silk S, Goyal SK. PO-05-224 Real world incidence of device-related thrombus with Watchman FLX PRO device. Heart Rhythm. 2025;22(4):S561. doi:10.1016/j.hrthm.2025.03.1398













