

Block the Bleed: Management of Coronary Perforation Using a Single 7F Guide Catheter
© 2026 HMP Global. All Rights Reserved.
Any views and opinions expressed are those of the author(s) and/or participants and do not necessarily reflect the views, policy, or position of the Journal of Invasive Cardiology or HMP Global, their employees, and affiliates.
J INVASIVE CARDIOL 2026. doi:10.25270/jic/26.00088. Epub April 9, 2026.
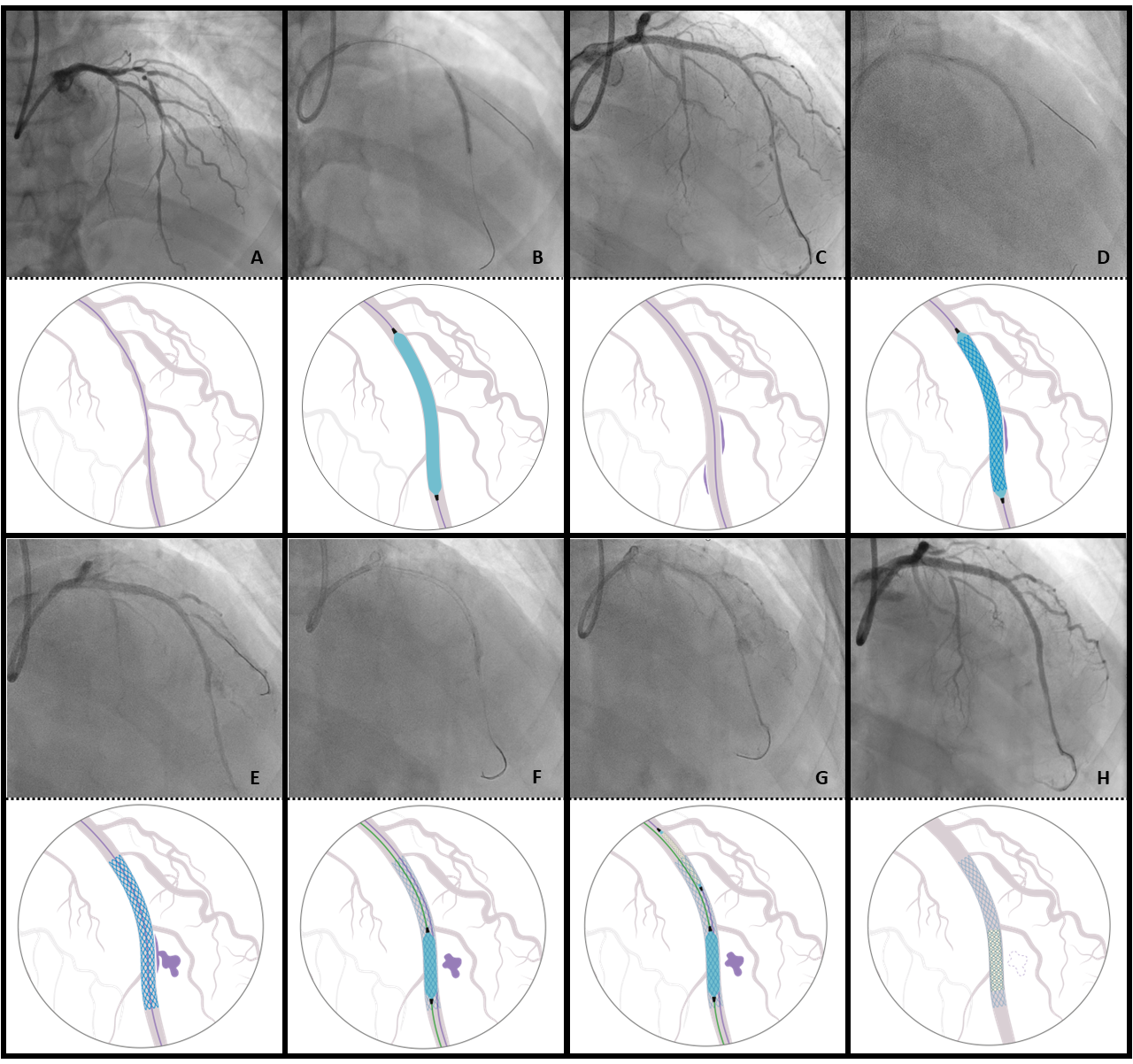
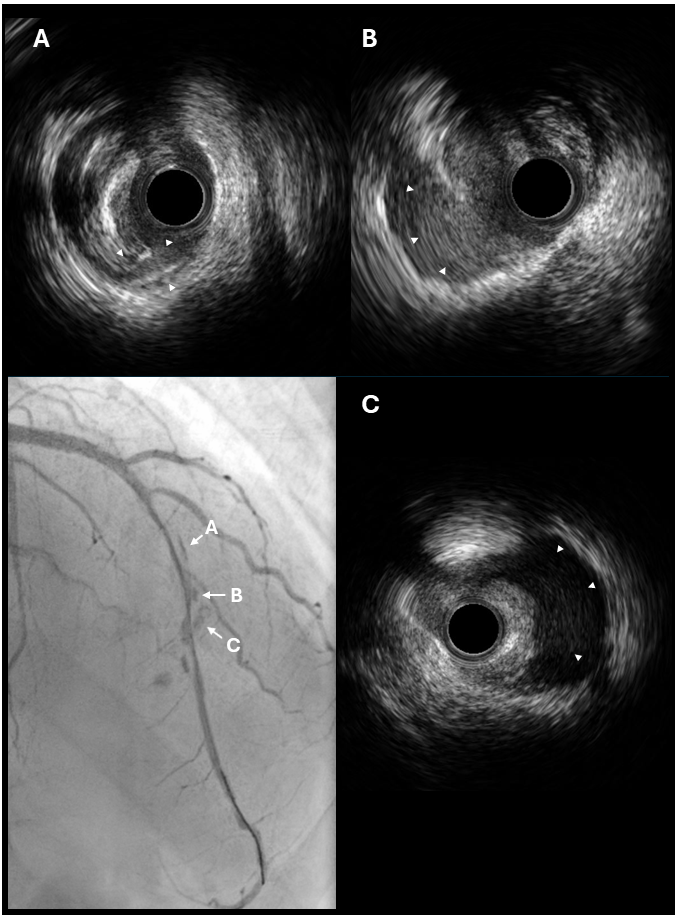
A 62-year-old man with unstable angina underwent coronary angiography (Figure 1A), revealing diffuse disease of the left anterior descending artery (LAD). A 7F 3.5 ExtraBackup Launcher guide catheter (GC) (Boston Scientific) was advanced via radial access. Lesion preparation with noncompliant balloons up to 3.5 mm at high pressure (Figure 1B) resulted in a type C dissection with persistent extraluminal contrast staining (Figure 1C, Video 1), confirmed on intravascular ultrasound (Figure 2, Video 2).
A 3.5 x 40-mm drug-eluting stent was implanted in the mid-LAD (Figure 1D), and subsequent contrast injection revealed an Ellis III perforation (Figure 1E). The stent balloon was re-advanced and reinflated to tamponade the bleeding. A second guidewire was advanced in parallel, and a shorter 3.5 x 15-mm balloon was used as a blocking balloon (Figure 1F). A 2.5 x 24-mm BeGraft covered stent (Bentley) was successfully delivered to the perforation site through the same 7F GC (Figure 1G). The blocking balloon and second wire were removed, and the covered stent was deployed, sealing the perforation (Figure 1H). The patient remained hemodynamically stable without pericardial effusion.
Coronary perforation is a life-threatening complication of percutaneous coronary intervention, requiring prompt recognition and management. The traditional “ping-pong” dual-GC technique is highly effective but time consuming and requires obtaining a second access in an emergency setting, which may increase the risk of vascular access-related complications.
A single 8F GC approach has been described, but this is not feasible with routine transradial access.1 This case demonstrates the feasibility and effectiveness of the “block-and-deliver” technique using a single 7F GC and a single-layer covered stent (≤ 4 mm), enabling rapid resolution of coronary perforation while avoiding the need for additional vascular access.
Affiliations and Disclosures
Laura Novelli, MD1; Jorge Sanz-Sanchez, MD, PhD2,3; Lea Usaj, MD4; Gabriele Luigi Gasparini, MD1
From the 1IRCCS Humanitas Research Hospital, Rozzano-Milan, Italy; 2Hospital Universitari i Politecnic La Fe, Valencia, Spain; 3Centro de Investigación Biomedica en Red (CIBERCV) – Madrid, Spain; 4Izola General Hospital, Izola, Slovenia.
Acknowledgments: The authors thank Vascular Perspective for their graphic design contribution.
Disclosures: The authors declare no conflicts of interest related to the content of this paper.
Consent statement: The authors confirm that informed consent was obtained from the patient for the intervention described in the manuscript and for the publication of their data, including any and all images.
Address for correspondence: Laura Novelli, MD, IRCCS Istituto Clinico Humanitas, Via Manzoni 56, 20089, Rozzano-Milan, Italy. Email: novelli.laura5@gmail.com
References
- Sandoval Y, Lobo AS, Brilakis ES. Covered stent implantation through a single 8-french guide catheter for the management of a distal coronary perforation. Catheter Cardiovasc Interv. 2017;90(4):584-588. doi:10.1002/ccd.27020















