


Case Presentation: Progressive Pediatric Hypothalamic Low-Grade Glioma With Newly Identified BRAF Fusion

Patient Case:
A now-14-year-old male initially presented at 32 months of age with a 6-month history of persistent nystagmus. Ophthalmologic exam was notable for mild optic disc pallor and decreased vision, with sensory nystagmus. An MRI was ordered, but in the interval, patient presented to the emergency department (ED) with new onset headache and vomiting; exam in the ED was notable for persistent nystagmus and limited vision; he had no café au lait macules, axillary or inguinal freckling, or other stigmata of neurofibromatosis type 1.
Head CT showed a large hypodense suprasellar mass with associated mild enlargement of the lateral ventricles with effacement of the sulci of the cerebral hemispheres. MRI similarly showed a large heterogeneous suprasellar/hypothalamic mass 5cm diameter mass, with avid heterogeneous enhancement and evidence of intratumoral hemorrhage. He underwent ventriculoperitoneal shunt placement and endoscopic third ventricular tumor biopsy. Pathology was consistent with low-grade astrocytoma. He underwent initial therapy with carboplatin and vincristine as per COG A9952. About 10 months into treatment, at the end of his 5th cycle of maintenance chemotherapy, he developed an anaphylactic reaction to carboplatin; treatment was discontinued at that time.
His subsequent course was notable for severe but stable vision loss. The tumor remained radiographically stable until he was 11 years old, when a routine MRI was notable for slight interval growth. In the absence of any corresponding worsening of his ophthalmological exam or other clinical changes, he was managed with continued close observation. Subsequent MRIs continued to show very slow interval growth, punctuated by periods of apparent stability.
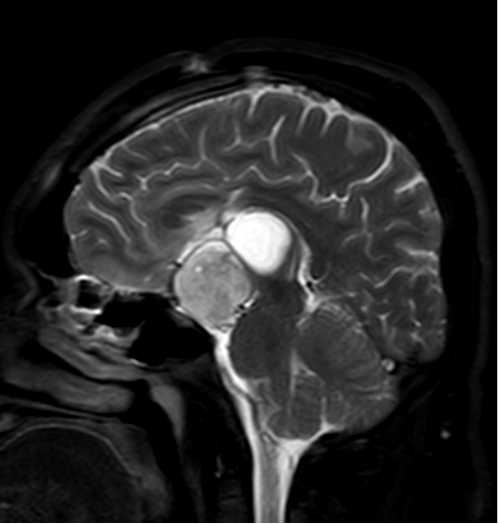
Now he is 14, and has begun to complain of worsening intermittent headaches, as well as new onset changes in short term memory. His ophthalmologic exam is unchanged. MRI shows further slow interval solid and cystic tumor progression, including new mass effect on the brainstem (Figure).
Targeted tumor sequencing, not clinically available when he was initially diagnosed, reveals a KIAA1549::BRAF fusion.
In discussion of reasonable next steps, several preferred options are presented to the patient and his caregivers.

