Silent Inflammation, Stormy Presentation: Bilateral Renal Artery Stenosis Secondary to Takayasu Arteritis
© 2025 HMP Global. All Rights Reserved.
Any views and opinions expressed are those of the author(s) and/or participants and do not necessarily reflect the views, policy, or position of the Journal of Invasive Cardiology or HMP Global, their employees, and affiliates.
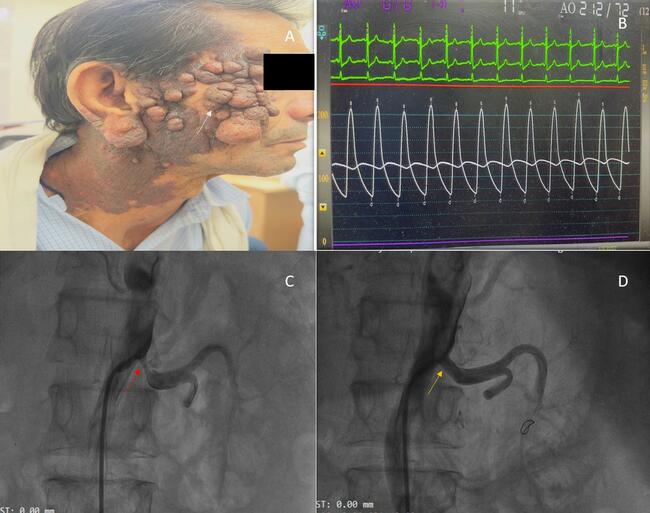
A 25-year-old man presented with 3 episodes of flash pulmonary edema in the past 2 months. Despite being on 4 antihypertensives, his blood pressure was 200/140 mm Hg. His serum inflammatory markers (erythrocyte sedimentation rate and C-reactive protein) were raised.
Computed tomography angiography of the abdomen revealed bilateral renal artery stenosis with 99% stenosis in the right renal artery and 90% stenosis in the left renal artery, with thickening of the abdominal aorta (Figure B) and the “double ring sign” (Figure A). A diagnosis of Takayasu arteritis type IV was made. Renal angiography confirmed the findings (Figure C and E) and, subsequently, the patient underwent bilateral renal angioplasty with a cutting balloon and a drug-coated balloon. The end result of the procedure was satisfactory with mild residual stenosis (Figure D and F) and a significant improvement in blood pressure. The patient was well controlled on a single antihypertensive at the 2-month follow-up.
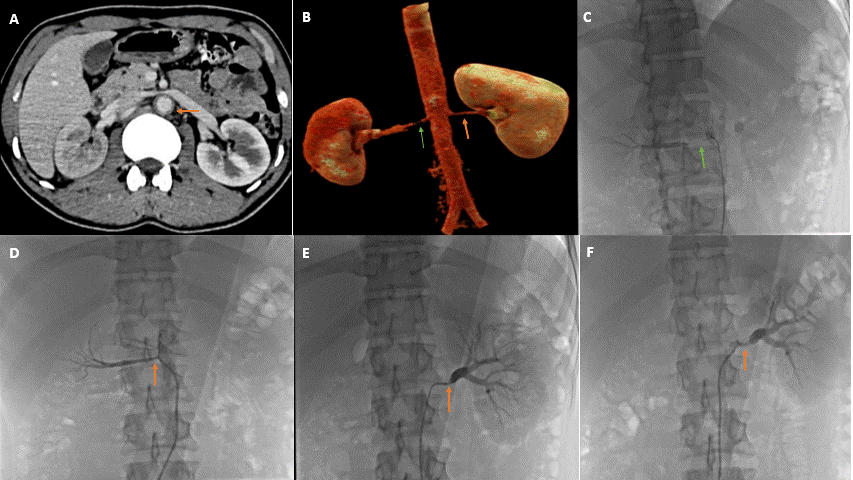
Takayasu arteritis is an idiopathic, large vessel vasculitis affecting the aorta and major branches. It has the highest affinity for the left subclavian artery; however, in the Indian population, abdominal aorta involvement is more common. The “double ring sign” is an important sign and marker of active disease (showing a hyperenhancing outer ring due to thickening of the medial and adventitial layers due to inflammation, and a hypoenhancing inner ring due to swelling of the intima and luminal narrowing). In light of ongoing disease activity and fear of stent restenosis in this case, stenting was deferred, and the patient underwent ballon angioplasty with acceptable results.
Affiliations and Disclosures
Devesh Kumar, MD, MRCP, DM1; Anil Kumar Choudhary, MD, DM2; Neeraj Rao, MBBS, MD2; Jai Purohit, MD, DM3; Somyata Somendra, MD, DM4
From the 1Department of Cardiology, Vardhman Mahavir Medical College and Safdarjung Hospital, New Delhi, India; 2Department of Cardiology, NIMS Medical College & Hospital, NIMS University, Jaipur, India; 3Department Of Cardiology, Shri Kalyan Govt. Medical College, Sikar, India; 4Department Of Cardiology, Eternal Hospital, Jaipur, India.
Disclosures: The authors report no financial relationships or conflicts of interest regarding the content herein.
Consent statement: The authors confirm that informed consent was obtained from the patient for the intervention described in the manuscript and for the publication of thereof, including photographs.
Address for correspondence: Anil Kumar Choudhary, MD, DM, Department of Cardiology, NIMS Medical College & Hospital, NIMS University, Jaipur, India. Email: chaudharyanil007ac@gmail.com