Subcutaneous Immuno-Oncology in Metastatic Melanoma: Evolving Treatment Delivery Beyond Efficacy
The Current Metastatic Melanoma Immuno-Oncology Landscape and the Unmet Need Beyond Efficacy
Melanoma is a highly aggressive skin cancer with a poor prognosis in its advanced stages. In the last decade, immune checkpoint inhibitors (ICIs) and targeted kinase inhibitors (TKIs) have revolutionized treatment and significantly extended patient survival, with the median survival reaching 5 to 6 years and the 10-year survival reaching 50% with combination ICI treatment.1
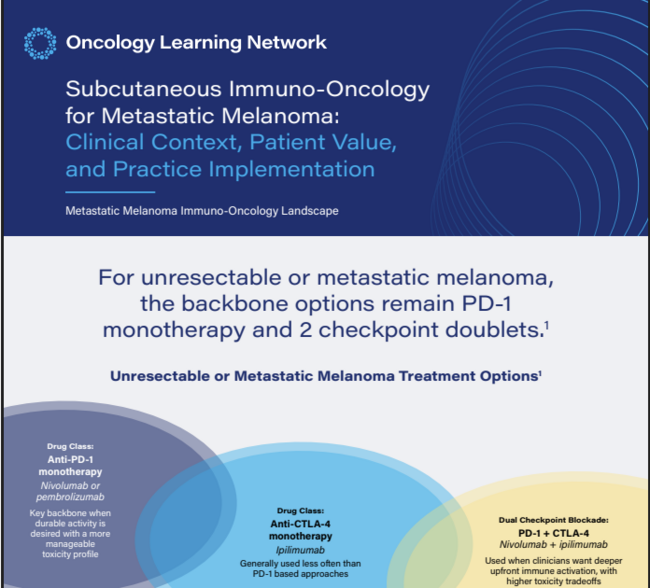
Today, the current immuno-oncology (IO) treatment landscape for metastatic melanoma is dominated by checkpoint inhibitors targeting programmed cell death protein 1 (PD-1), cytotoxic T-lymphocyte-associated protein 4 (CTLA-4), and lymphocyte activation gene 3 (LAG-3), which activate T-cell responses against tumors.1
Anti-PD-1 monotherapy, which includes nivolumab or pembrolizumab, is often used when clinicians want durable activity with a generally more manageable toxicity profile.2
Dual checkpoint blockade includes nivolumab plus ipilimumab as the PD-1/CTLA-4 option, and nivolumab plus relatimab as the PD-1/LAG-3 option.2
Nivolumab plus ipilimumab is often considered when the goal is deeper upfront immune activation, and the patient is fit enough for the added toxicity burden that may accompany CTLA-4–based intensification. Nivolumab plus relatlimab is an intermediate option that is more intensive than PD-1 monotherapy but generally less aggressive than the nivolumab/ipilimumab doublet.2,3
Anti-CTLA-4 monotherapy with ipilimumab remains another IO option and was the first immune checkpoint inhibitor approved for unresectable or metastatic disease, although it has generally shown lower response rates and less favorable survival outcomes than anti-PD-1 monotherapy.2,4,5
For stage II and stage III melanoma, neoadjuvant systemic therapy has become a more prominent part of management.6 This approach reflects the growing importance of earlier systemic intervention in patients at higher risk of recurrence.
The treatment choice is shaped by disease history, symptom burden, comorbidities, prior exposure, tolerance for immune-related adverse events, and the patient’s own priorities.7
With multiple preferred immunotherapy options available for melanoma, the goal is to select the appropriate therapy for the patient, taking into consideration treatment intensity, toxicity, quality of life, and treatment burden. One aspect of treatment burden to consider is how the treatment is delivered and the logistics surrounding getting the treatment.8
For many patients, factors such as travel time, parking, repeated infusion-center visits, venous access, caregiver scheduling, missed work, time away from family responsibilities, and the emotional fatigue of spending recurring blocks of time in the clinic can influence adherence, satisfaction, and the perceived sustainability of treatment, even when efficacy is not in question.8
In that sense, the route of administration may become part of the overall value proposition of treatment. As oncologists think about what still needs to improve in melanoma care, the answer increasingly includes not only better biologic outcomes but also a better fit between a highly effective therapy and the realities of everyday practice.9
Subcutaneous Immuno-Oncology Options: Where They Fit and Why They Are Credible
With multiple effective IO options in metastatic melanoma, delivery and logistical burden are increasingly important considerations. Subcutaneous (SC) IO options may offer a practical alternative by reducing time in clinics while maintaining the role of familiar PD-1–based therapy.
As of March 2026, 2 SC checkpoint inhibitor options are approved for the treatment of metastatic melanoma: nivolumab plus hyaluronidase-nvhy and pembrolizumab plus berahyaluronidase alfa-pmph. These SC IO options provide an alternative route of administration that is within accepted standards of care.10,11
In melanoma, nivolumab plus hyaluronidase-nvhy is indicated for12:
-
Monotherapy for adjuvant treatment of stage IIB/C, III, and IV melanoma in adult and pediatric patients
-
Monotherapy for unresectable or metastatic melanoma, including after intravenous (IV) nivolumab + ipilimumab in the maintenance setting, in adult and pediatric patients 12 years and older
However, it is not indicated for concurrent use with IV ipilimumab for metastatic melanoma.
Pembrolizumab plus berahyaluronidase alfa-pmph is indicated for13:
-
Monotherapy for adjuvant treatment of stage IIB/C or stage III melanoma in adult and pediatric patients
-
Monotherapy for unresectable or metastatic melanoma in adult patients
The data supporting the approval of these SC IO options is best viewed as formulation-bridging evidence rather than specific head-to-head trial data for melanoma. Instead, the regulatory standard focused on whether SC delivery produced comparable pharmacokinetics, efficacy, and safety compared to the known IV nivolumab or pembrolizumab.
For SC nivolumab, CheckMate 67T was a phase 3, open-label, randomized noninferiority study in clear cell renal cell carcinoma receiving SC administration of a flat dose of 1200 mg nivolumab coformulated with recombinant human hyaluronidase 20 000 units every 4 weeks or IV administration of 3 mg/kg nivolumab every 2 weeks. It met coprimary pharmacokinetic endpoints and also demonstrated a noninferior objective response rate, with a safety profile consistent with IV nivolumab.14
For SC pembrolizumab, MK-3475A-D77 was a phase 3, open-label, randomized noninferiority study in metastatic non-small-cell lung cancer. Patients received SC pembrolizumab 790 mg every 6 weeks or IV pembrolizumab 400 mg every 6 weeks (18 cycles), in combination with platinum-doublet chemotherapy. It similarly showed noninferior exposure and trough concentrations, with efficacy and safety profiles consistent with IV pembrolizumab.15 Together, these data support the idea that SC delivery maintains confidence in the active drug backbone.
The noninferiority trial data for nivolumab + hyaluronidase-nvhy and pembrolizumab + berahyaluronidase alfa-pmph have established that SC delivery of nivolumab or pembrolizumab is as effective and safe compared to their IV forms, offering a practical alternative for patients with metastatic melanoma.
Advantages of Subcutaneous Immuno-Oncology for Patients
The primary patient-level advantage of SC IO is that it can reduce the time spent receiving treatment, which is one of the least appreciated burdens of metastatic melanoma treatment. SC nivolumab is administered in approximately 3 to 5 minutes, compared with a 30-minute IV nivolumab infusion.16 SC pembrolizumab is administered in about 1 minute for the dose given every 3 weeks and about 2 minutes for the dose given every 6 weeks.11 In patients' real-life experience with cancer treatment, this time difference can be very meaningful. Additionally, logistical burdens such as transportation, caregiver arrangements, missed work, parking, waiting, venous access, and repeated infusion-center visits associated with IV administration contribute to patients' treatment burden. While a shorter administration route does not eliminate these burdens, it can help reduce them.9
Direct melanoma-specific preference data for SC checkpoint inhibitors are still emerging. However, the broader oncology literature consistently shows that patients and healthcare providers (HCPs) often prefer SC administration when efficacy is comparable, largely because of reduced time burden and convenience. A 2024 systematic review found substantially higher patient and HCP preference rates for SC over IV administration across oncology settings and lower time and resource use with SC delivery.17
In terms of tolerability and practical experience of SC delivery, the most frequently reported symptoms from SC administration were injection-related redness, itching, pricking (needle) pain, and stinging/tingling pain, in a qualitative interview study of 43 participants in non-small cell lung cancer, renal cell carcinoma, unresectable or advanced metastatic melanoma, hepatocellular carcinoma, or colorectal cancer trials.18 In the same study, 91% of participants expressed a preference for SC treatments over IV treatments, compared to 9% who preferred IV treatments, highlighting a strong patient preference for SC delivery. Injection-site reactions do occur with SC delivery, but in CheckMate 67T and MK-3475A-D77, they were generally low-grade and transient.14,18
With SC IO options offering time and convenience benefits while maintaining the efficacy of the therapeutic backbone, they provide patients with options that can better fit with their needs.
Implementing SC IO in Practice: Operationalizing Value in the Real World
Even when clinicians recognize the value of SC administration of IO treatment for patients with metastatic melanoma, implementation can falter when practices lack a clear path to operationalizing it. Operational success depends on addressing the central question, “How can subcutaneous administration of IO be operationalized in a way that preserves clinic flow and minimizes disruption?”
A strong starting point is a cross-functional working group that includes physicians, nurses, pharmacists, pharmacy technicians, scheduling leaders, infusion leadership, administrative staff, and financial or authorization teams. Group members should be educated about and understand the patient and system benefits of switching to SC administration. This group can review all functions, systems, and processes that may be impacted by the change: order entry, medication storage, preparation and handling, chair allocation, nursing technique, scheduling templates, patient education, local reaction management, and documentation standards.19
From a clinic-flow perspective, SC administration may shorten visit length, creating more scheduling flexibility for both patients and clinics. Shorter chair time can improve infusion center throughput, allowing infusion chairs to be used for other treatments. That can be valuable in busy oncology settings where chair time is constrained, and infusion resources must be reserved for regimens that truly require prolonged administration. Pharmacy operations may also become more efficient by reducing compounding time and eliminating the need for IV bag preparation. Clinics may need logistical updates to storage processes, staffing workflows, patient selection criteria, and coordination across nursing, pharmacy, and financial teams. Financial and authorization workflows can determine feasibility, making early coordination with authorization and financial advocacy teams important.20
Nursing preparation is especially important because SC oncology administration requires competence in site selection, site rotation, injection pacing, pinch technique, body mechanics, patient communication, and response to local injection reactions. Teams also need clarity on observation practices, adverse event documentation, and how patients are selected for the SC route.20
References
- Kato H. Drug therapy for melanoma: current updates and future prospects. Cancers (Basel). 2026;18(3):382. doi:10.3390/cancers18030382
- PDQ® Adult Treatment Editorial Board. Melanoma Treatment (PDQ®)–Health Professional Version. National Cancer Institute. Updated May 2, 2025. Accessed March 30, 2026. https://www.cancer.gov/types/skin/hp/melanoma-treatment-pdq#_1
- Kooshkaki O, Derakhshani A, Hosseinkhani N, et al. Combination of ipilimumab and nivolumab in cancers: from clinical practice to ongoing clinical trials. Int J Mol Sci. 2020;21(12):4427. doi:10.3390/ijms21124427
- Allen-Tejerina AM, Giannakis P, Ho Lai Yau T, Hillyar CRT, Rallis KS. Immune checkpoint inhibitors in malignant melanoma: anti-PD-1, anti-CTLA-4 and anti-LAG-3 therapies. Curr Oncol Rep. 2026;28(1):23. doi:10.1007/s11912-026-01750-1
- Weiss SA, Wolchok JD, Sznol M. Immunotherapy of melanoma: facts and hopes. Clin Cancer Res. 2019;25(17):5191-5201. doi:10.1158/1078-0432.CCR-18-1550
- Farma JM, Olszanski AJ, Messina JL, Sondak VK. Annals of Surgical Oncology Practice Guidelines series: adjuvant and neoadjuvant therapy for melanoma. Ann Surg Oncol. 2025;32(1):3-11. doi:10.1245/s10434-024-16418-y
- Kreft S, Bosetti T, Lee R, Lorigan P. Selecting first-line immunotherapy in advanced melanoma: current evidence on efficacy across diverse patient populations. EJC Skin Cancer. 2025;3:100285. doi:10.1016/j.ejcskn.2025.100285
- Lin K, Kagalwalla S, Gupta A. Characterizing and addressing the financial, time, and administrative burdens of cancer and its care. Curr Treat Options Oncol. 2025;26(12):1078-1085. doi:10.1007/s11864-025-01358-w
- Bittner B, Richter W, Schmidt J. Subcutaneous administration of biotherapeutics: an overview of current challenges and opportunities. BioDrugs. 2018;32(5):425-440. doi:10.1007/s40259-018-0295-0
- Bristol-Myers Squibb Company. Opdivo®. Accessed March 30, 2026. https://www.opdivohcp.com/
- Merck & Co, Inc. Keytruda Qlex™. Accessed March 30, 2026. https://www.keytrudahcp.com/qlex
- Opdivo Qvantig. Prescribing information. Bristol-Myers Squibb Company; 2025.
- Keytruda Qlex. Prescribing information. Merck & Co, Inc; 2026.
- Albiges L, Bourlon MT, Chacón M, et al. Subcutaneous versus intravenous nivolumab for renal cell carcinoma. Ann Oncol. 2025;36(1):99-107. doi:10.1016/j.annonc.2024.09.002
- Felip E, Rojas CI, Schenker M, et al. Subcutaneous versus intravenous pembrolizumab, in combination with chemotherapy, for treatment of metastatic non-small-cell lung cancer: the phase III 3475A-D77 trial. Ann Oncol. 2025;36(7):775-785. doi:10.1016/j.annonc.2025.03.012
- Bristol-Myers Squibb Company. Subcutaneous treatment option. Accessed March 30, 2026. https://www.opdivohcp.com/efficacy/subcutaneous-administration
- George S, Bourlon MT, Overman MJ, et al. Systematic literature review of intravenous versus subcutaneous administration of oncology therapies: a clinical, economic and patient perspective. Cancer Treat Rev. 2025;139:102974. doi:10.1016/j.ctrv.2025.102974
- Skalicky A, Bennett B, Raimbourg J, et al. Patient experience of medication administration and development of a Patient Experience and Preference Questionnaire (PEPQ) for patients with advanced or metastatic cancer. Front Pharmacol. 2024;15:1310546. doi:10.3389/fphar.2024.1310546
- Boudreau A. Practical considerations for the integration of subcutaneous targeted therapies into the oncology clinic. Can Oncol Nurs J. 2019;29(4):267-270.
- APSHO Case-Based Learning: Best Practices in the Adaptation of Subcutaneous Injection Drug Delivery in Cancer. Advanced Practitioner Society for Hematology and Oncology; 2025.
© 2026 HMP Global. All Rights Reserved.